

NEWS
IBD and Eating Disorders: Control, Fear, and Survival
by Michelle Garber (California, U.S.A.)

An empty pink-orange plate with a knife and fork on a white background. The plate and utensils have some food remnants left on them, as though they were recently used.
Content Warning: this article discusses eating disorders and topics such as food restriction, binge eating, and body dysmorphia.
For as long as I can remember, food has never been just food. It has been comfort, control, fear, shame, and even the sole measure of my worth. I began struggling with disordered eating as a child, long before I knew anything about Inflammatory Bowel Disease (IBD) or ulcerative colitis—the chronic illness that would later reshape my relationship with my body all over again.
My earliest battle was with anorexia nervosa. I was only around twelve when I began restricting food, counting every calorie, and chasing the illusion of control that came with watching the number on the scale drop. Almost no one knew. The secrecy was part of the sickness—the quiet shame that thrived in silence. It felt safer that way. In a strange way, that shame felt familiar when I was later diagnosed with IBD. Both conditions carried a stigma. Anorexia was whispered about in terms of vanity and control, and conversations about IBD were avoided altogether because they involved the "uncomfortable" topics of bowels, bathrooms, and bodies.
By my senior year of high school, I had relapsed in terms of my anorexia. With prom and graduation approaching, I wanted to "feel confident" in my own skin, but my desire for control quickly turned into obsession again. I convinced myself that going vegan and gluten-free would "clear my acne" and "make me healthier." When it didn't, though, I continued anyway. I continued because I had found something else: the rush of watching the scale drop again. I told myself that it was about health, but deep down, it was about control, perfection, and fear.
When COVID hit, prom and graduation vanished, but my eating disorder didn't. Even though I eventually abandoned the vegan diet, my restriction continued. My hair began falling out in clumps. I was so weak that I needed to be pushed in a wheelchair on family walks and through grocery store aisles. Still, I clung to denial, blaming my fatigue and hair loss on my thyroid. I wasn't ready to admit that I was sick again—not from a medical condition, but from the same mental illness I thought I had conquered.
The human body can only endure starvation for so long before it rebels. Mine did—violently. The pendulum swung from restriction to bingeing. Binge eating disorder involves recurring episodes of eating large amounts of food rapidly, often to the point of physical discomfort, accompanied by feelings of loss of control and guilt afterward.
That was my reality. I gained weight rapidly and felt completely out of control. If anorexia gave me a false sense of control over my life, binge eating disorder stripped it away. I swung from one extreme to another, and both made me miserable. When the weight gain triggered the same familiar self-loathing, I spiraled right back into an anorexia relapse again—a vicious cycle of control and chaos that consumed years of my life.
Eventually, my body began to fail. My heart rate slowed to dangerously low levels. For the first time, I allowed myself to admit the truth: I did not want to die. Recovery, for me, began not with love for my body, but with the simple desire to stay alive.
I began eating again, slowly and carefully. On paper, it looked like recovery—my calories were adequate and my body was functioning. Mentally, though, I was still trapped. I measured every ounce of food, logged every calorie, and spent hours preparing meals to ensure perfect precision. I told myself that it was about maintaining my metabolism, but it was still about fear—the fear of losing control, the fear of gaining weight, and the fear of trusting my body.
Even when I was "eating normally," my life revolved around food. I avoided restaurants unless they posted nutrition information online. I sometimes ordered takeout, only to bring it home and weigh it myself. I had simply traded starvation for obsession. I thought that I had my eating disorder under control, but in truth, it still controlled me.
Around this time, I began experiencing digestive symptoms: constipation, vomiting, reflux, and pain. I now believe that my disordered eating—the pendulum swing from restriction to bingeing, my extremely high insoluble fiber intake in order to eat high volumes of food with the least amount of calories, and my reliance on laxatives due to my food restriction—played a role in triggering my ulcerative colitis, along with the mental/emotional stress caused by it all.
When I was finally diagnosed with IBD, I thought that my disordered eating would take a back seat. I was wrong. Chronic illness can be fertile ground for eating disorders to grow. The constant focus on diet, the fear of flares, and the unpredictability of symptoms can reawaken old patterns of control and restriction.
In the hospital, I was prescribed prednisone and given a list of "safe foods." Back home, I stuck to that list religiously. Underneath it all, though, my old compulsions still resurfaced. I limited not just insoluble fiber, spicy foods, dairy, and alcohol—which are common triggers during flares—but also carbs, sugars, and sodium. This was due to the fear of prednisone-induced weight gain—the water retention, "water weight," or "moon face" that prednisone could cause. I told others that it was about inflammation, but in truth, I was relapsing again—this time under the socially acceptable cover of a "medical diet."
This is one of the hardest truths about eating disorders and IBD: the overlap between medical management and disordered eating behaviors is often blurred. The two can feed each other in quiet, dangerous ways.
IBD can create new patterns of disordered thinking in people who have never struggled with eating disorders before. This is because when your body betrays you like it does with IBD, food becomes (or at least feels like) one of the few things that you actually can control. Plus, when your weight fluctuates rapidly—sometimes losing as much as thirty pounds in a week and then regaining it soon after—it can completely destabilize your sense of self.
For those with body dysmorphia or a history of disordered eating/anorexia, this is especially dangerous. There's no such thing as "small enough" in the mind of someone with an eating disorder. Seeing a "low" number on the scale (even when it's caused by illness) can increase your dopamine and ignite the urge to chase that number, again and again. I remember logically understanding that my low weight during my flare was unhealthy, but emotionally, I still felt anger and panic when the scale went up after treatment. Prednisone's mood swings certainly didn't help with this either—I was at war with both my mind and body.
Now, in remission from IBD, I can finally say that I am also in recovery from my eating disorders. Even so, recovery (like remission) is never as simple as it sounds.
Even in remission, disordered eating behaviors can quietly persist. For many of us with IBD, it shows up as hypervigilance around food: the fear of new foods, the obsession with "safe" meals, or the guilt after eating something "off-plan." It can look like avoiding social events involving food, fixating on weight fluctuations caused by steroids, or tying self-worth to whether symptoms worsen after a meal. These behaviors can masquerade as "caution," but they're often echoes of deeper fear—the fear of pain, the fear of loss of control, and the fear of being sick again.
The parallels between IBD and eating disorders are striking. Both involve an uneasy relationship with the body—a sense that your own physical self has turned against you. Both can make you feel powerless, trapped, ashamed, and isolated. Both can lead to cycles of control and surrender, as well as perfectionism and self-punishment. And both are often invisible to others, hidden behind a mask of composure and "doing fine."
Today, my relationship with food is no longer about control—or at least, I'm trying to keep it that way. I eat intuitively when I can, forgive myself when I can't, and I remind myself that nourishment is not a punishment or reward; it's an act of care. My body has been through battles most people can't see—battles maybe I never even noticed. My body deserves gentleness, not control or being told that it isn't "good enough." Yes, my body may have not been the kindest to me over the years, but I also haven't been the kindest to it in return. While my body may have betrayed me in some ways due to my IBD, it has also gotten me through my IBD, my eating disorders, and so much more. My body is not my enemy. My IBD is not my enemy. My weight is not my enemy. How I look in the mirror one day versus how I look in the mirror the next is not my enemy.
Living with both IBD and a history of eating disorders means constantly walking the line between vigilance and obsession, as well as between self-protection and self-harm. Even so, I've learned that healing is not about never struggling again—it's about recognizing when the struggle starts to whisper and, this time, choosing to listen with compassion instead of control.
For more information on disordered eating & IBD, check out this patient-created resource by the ImproveCareNow Patient Advisory Council.
Image from @jogaway on Unsplash.
To See What Cannot Be Seen: Living with Chronic Pain and IBD
by Michelle Garber (California, U.S.A.)

A blue and black striped background, with the word “PAIN” spelled out in medications.
When most people hear the word "remission," they imagine relief, a clean slate, and the end of suffering. For those of us living with Inflammatory Bowel Disease (IBD), remission is supposed to mean that we can finally be free of the pain that controlled our lives and simply breathe again. Unfortunately, for so many IBD patients, remission doesn't mean that the pain disappears. Rather, our pain changes form. Our pain becomes quieter, more private, and more invisible. It becomes the kind of pain that can exist in silence. The kind of pain that may not scream for help, yet it still whimpers day and night. The kind of pain that is easy to be overlooked while the rest of the world assumes you're fine.
Chronic pain is one of the most misunderstood aspects of IBD. It lingers long after flares fade, threading through your days in ways that are impossible to explain. It's invisible, yet constant. It's being in pain every single day, but learning to function anyway because you have no other choice. Chronic pain has become a part of my life—like a ringing in my ears that I've had to learn to ignore. I've learned to appear "fine" because visible pain tends to make others uncomfortable, and because I've discovered that admitting the truth often leads to dismissal. I have become so adept at masking my pain that I've become fluent in pretending. Pretending that I'm not silently calculating how much longer I can keep standing before the pain in my abdomen forces me to sit down. Pretending that the subtle grimace that escaped when I moved the wrong way was just a product of my "resting b*tch face." And pretending that "pain" is no longer in my vocabulary.
The pain of IBD patients also commonly goes unrecognized by medical professionals because the traditional 1-10 pain scale was not built for those living with chronic pain. For example, if I tell a doctor that my pain is at a "6/10," they may interpret that as "moderate discomfort." For those without IBD or chronic pain, though, my "6" might be their "10." Our baseline is simply so different from those without chronic illness/chronic pain, therefore making the standard 1-10 pain scale almost meaningless for us. This can have dangerous consequences as pain is typically the body's signal that something is wrong. When we are constantly experiencing pain, it can be difficult to determine whether it's "significant enough" to seek help or whether it's just our "new baseline." The fact of the matter is that any pain should be and is "significant enough," but we've been conditioned to not view it as such. We've been conditioned to accept a new and distorted "baseline level of pain" due to our illness, when those without chronic pain are not encouraged to do the same. Therefore, it can be hard for both us and medical professionals to know when something is "wrong," creating the potential for treatment delays, disease progression, prolonged suffering, and—depending on the illness—even fatal consequences.
Living with chronic pain often means learning to downplay your pain. No matter how much pain I'm in, I never rate my pain as a "10." I rarely even rate it as an "8" or a "9" because I know what happens when I do. I've seen "the look." It's that flicker of suspicion that crosses a medical provider's face when you say you're in severe pain, but you don't exactly "look" like it. I have felt the shift in tone when my honesty is mistaken for medication-seeking or when my tears are assumed to be those of ‘crocodiles.’ Because as it has been made quite clear by many medical professionals, if you don't have overwhelmingly visible evidence of your pain, then it must be exaggerated. Or, you must have a mental illness since "it's just anxiety," and "it's all in your head." So, like many others, I minimize my pain. I say that it's a "4" or "5." I'll tell doctors that my pain is manageable, even when it's often very much not.
The stigma of simply wanting relief is one of the cruelest aspects of IBD and chronic pain. The truth is, it's terrifying to need help in a system that might not believe you. IBD also presents unique challenges when it comes to pain management. Nonsteroidal anti-inflammatory drugs (NSAIDs) are usually off-limits because they can actually trigger flares. Opioids, while sometimes the only medications strong enough to even touch the pain, are approached with understandable caution due to their risks (i.e. the potential for constipation, dependency, and/or substance use disorder). As a result, we're often left to "cope." We're told to meditate, breathe, use heating pads so often that we burn ourselves, and/or use methods of distraction while our insides feel as though they're literally being twisted inside-out. If we're lucky, we might just get a pamphlet or a link to a video explaining these coping mechanisms. We're essentially almost abandoned by most medical providers as they expect us to endure significant pain without the use of effective pain relief options.
Don't get me wrong, these coping skills can help, but they certainly don't erase our pain. They just make it more bearable. Over time, the constant strain of pushing through the pain can wear down even the strongest person—the person who has "been through it all" and has a "high pain tolerance." Chronic pain doesn't just live in the body. Chronic pain infiltrates the mind and can chip away at one's patience, hope, and even will to keep fighting.
Yet, I understand why providers are cautious when it comes to pain management because I've seen the other side of it too. I currently work at a substance use disorder treatment center as a soon-to-be therapist. I've noticed that many clients' struggles with substances began in the same place: pain. Some struggled with physical pain, some with emotional pain, and many with both. Some clients even suffered from chronic illness(es)/injuries, were told that there was nothing that could be done for their pain, and were never provided with any sort of pain relief by their doctors. Others were prescribed opioids for a while and were then abruptly cut off from them by their medical providers. Much of their substance use history echoes the desperation that many IBD patients have also experienced—the desperation to simply function. The desperation to hold down a job and just get through the day. The desperation to be able to sleep through constant throbbing and aching. The desperation to escape one's pain for "just five minutes." The desperation to just be.
These stories serve as a reminder that pain affects so much more than what meets the eye. That's why it hurts so deeply when our pain is minimized by doctors, friends, family members, partners, and even by ourselves. We tell ourselves that our pain isn't as bad as it feels, while we're quietly counting the minutes until we can lie down. We tell others that we're "fine" because we don't want to be seen as "fragile" or "dramatic." We tell doctors lower numbers on the pain scale so that they'll take us seriously. Many of us would rather suffer quietly than risk being labeled. We learn to mask pain so well that even those closest to us never usually realize the strength it takes for us to just get out of bed.
Masking pain comes at a cost, though. Each time we minimize our pain, we invalidate our own experience. We erase a little bit of our own truth, piece by piece—a small but painful act of self-betrayal that we've been conditioned to commit in order to be believed. Masking pain also isolates us. It makes our struggle invisible, and in doing so, it allows others—including medical professionals—to not be able to see the undeniable pattern of IBD patients with chronic pain.
Pain is not just a symptom. It's a lived experience that profoundly shapes our relationships, our work, our self-worth, our future, and our sense of identity. For example, we might pursue occupations that don't require physical labor, and we might choose living environments that are close to our caregivers/doctors, have bathtubs over showers, and lack staircases. For those of us living with a chronic illness, pain becomes part of who we are—not because we want it to, but because it demands to be acknowledged.
Living with chronic pain and IBD means existing somewhere in a space between endurance and exhaustion. Between being believed and being dismissed. It means learning to hold compassion for yourself, even when the world doesn't. It means carrying an invisible burden that requires extraordinary strength to bear, even though it feels as though you have no strength left to do so. It means showing up—for others, for yourself, and for life itself—often without anyone realizing just how much effort it all takes.
That quiet persistence is something that I have come to admire deeply, both in myself and in others who live this reality. Because even when our pain is invisible, our resilience is not. It serves as a powerful testament to every person who keeps going despite their own body making the simplest things feel impossible. And even though our pain may be a part of who we are, our resiliency proves that it is certainly not all of who we are. We are so much more than our pain and our illness.
Still, our pain deserves to be acknowledged. Our stories deserve to be believed. Our healthcare system must learn to see what cannot be seen—not to just treat the illness, but to honor the full human experience of actually living with it.
Therefore, we need a better way to talk about chronic pain, especially in regards to IBD. We need providers to understand that our "normal" is not their "normal." That just because we appear to be "fine" does not mean that we are not suffering. That pain in remission is real. And that asking for pain relief isn't manipulation—it's survival.
Living with chronic pain and IBD means learning to navigate a world that often doubts what it can't see. But we exist, and our pain is valid. It's time for the system and the world to finally see us because if you look hard enough, you'll see that our pain is actually not as invisible as it seems—it just continues to go unseen.
Image by @gnikomedi on Unsplash.
Mental Health & IBD Series
by the 2025 CCYAN Fellows

A graphic of the earth, with black text reading “IBD and Mental Health: Global Perspectives.”
This month, some of our fellows worked together to share perspectives on mental health and IBD. Check out their articles and videos on this topic below!
Insights from Beamlak (Ethiopia), Aiswarya (India), and Lexi (U.S.A.)
Living with inflammatory bowel disease (IBD) is never just about physical symptoms. It impacts mental health, education, relationships, and self-worth. For many patients, the emotional toll can be as heavy as the physical pain. We came together to explore the connection between IBD and mental health, and each of us shares a different perspective, facts, lived experiences, and personal reflections. Together, they form one message: mental health in IBD care is not optional, it is essential. We wanted to show that IBD is both a physical and mental health journey. Data highlights the need for better systems of care, and personal stories remind us of the resilience and strength it takes to keep moving forward. Together, we call for greater awareness, compassion, and support for every person living with IBD.
Read their perspectives:
Facts we Can’t Ignore - Lexi
Diagnosis is a Light, not a Lampshade - Aiswarya
“Let it” - My Rule for Living with IBD - Beamlak
Insights from Akhil (India) & Alexis (U.S.A.)
Akhil & Alexis (alongside 2022 CCYAN Fellow Maalvika & CCYAN’s Program Manager Rosa) presented about the intersections of Chronic Illness, Mental Health, and Cultural Considerations at the 2025 Bridging Voices, Building Futures: Youth Innovation in Mental Health Conference (hosted by Generation Mental Health). View the presentation below:
Check out more of our 2025 fellow’s articles and videos on other mental health topics:
What it’s Like Working Through Phobias - Kaitlyn Niznik
Through (on Stigma, Shame, and Talking about IBD) - Michelle Garber
God of Small Things: A Crohn’s View (on Stigma and Connection) - Rifa Tusnia Mona
IBD & Grief by Akhil Shridhar
Internalized Stigma in IBD, Mental Health, and Quality of Life by Aiswarya Asokan
Mental Health & IBD (An Infographic) by Lexi Hanson
The Facts We Can’t Ignore (Mental Health & IBD Series)
by Lexi Hanson (Missouri, U.S.A.)

A speckled grey granite countertop, with black scrabble tiles spelling out “Mental Health Matters.”
According to the American Gastroenterological Association (AGA), 35–36% of IBD patients report anxiety or depression—far above national averages. Yet, too often, providers prioritize physical health while overlooking mental health needs. Supporting mental health is not a luxury for IBD patients—it is a necessity.
What are some supports that can make a difference for Young Adult IBD patients?
Embedding mental health professionals (psychologists, social workers) in IBD care teams.
Routine mental health screening for young adults.
Coping toolkits to build self-advocacy, communication skills, and emotional resilience.
Extending transition support to age 25, not just 18–20.
Availability of peer and lived-experience communities for validation and advice.
Access to reliable information tools about nutrition, travel, accommodations, relationships, fatigue, and brain fog.
IBD-aware university services: bathroom access, class accommodations, and counseling.
Policy reforms to ease insurance challenges and improve navigation.
Education on ADA rights and workplace accommodations.
Self-compassion training to protect mental health.
Check out Lexi’s July post for more facts about Mental Health & IBD!
Photo from Unsplash.
“Let It” — My Rule for Living with IBD (Mental Health & IBD Series)
by Beamlak Alebel (Addis Ababa, Ethiopia)

Two hands reach towards one another. One is handing a black paper heart to the other outstretched hand.
Living with Inflammatory Bowel Disease (IBD) is a journey no one truly understands unless they’ve walked it themselves. It changes your body, your mindset, your lifestyle — and even your identity. Over the years, I’ve discovered a rule that helps me rise above the noise, pressure, and pain:
“Let It…”
It reminds me to stop fighting what I can’t change and instead make peace with it — to keep breathing, keep moving, and most of all, keep living.
Let It Be What It Is
IBD is unpredictable. One day you feel okay; the next, you’re back in the hospital.
I remember one exam day when the classroom was overcrowded. I had followed every rule—no phone, fully prepared—but when I arrived, every desk was already taken. There was no seat left for me.
It wasn’t a flare. I had come ready to write the exam, but the conditions made it impossible. I felt angry and frustrated—I had put in the effort, yet I was turned away by circumstances beyond my control. Missing that exam hurt deeply, not only academically but also emotionally. Still, I whispered to myself: “Let it. Everything has a reason.”
Let People Say What They Want
“You don’t look sick.” “Are you sure it’s that serious?” People don’t see what happens behind closed doors — the fatigue, the pain, the hospital visits. Their words used to cut me, but I’ve learned: “I don’t need to prove my pain.”
Let Yourself Say No
There are foods I can’t eat, events I can’t attend, and expectations I can’t meet. I used to feel guilty for saying no, as if I was letting people down. Now I know: “Let yourself say no. It’s not weakness — it’s wisdom.”
Let Hope In
On the hard days, hope is my medicine. Sometimes all I can say to myself is: “Tomorrow is another day.” And that’s enough. Even a tiny spark of hope can carry me through the darkest moments.
Let Go of Pressure
IBD puts pressure on every part of life — physically, emotionally, and socially. I’ve let go of the need to be perfect. If my body tells me to rest, I listen. If I miss something important because of my health, I remind myself: “My health comes first.”
Let Life Be Easier
I no longer compare my life to those who seem to “have it all together.” My peace, joy, and success may look different, and that’s okay: “Let life be gentle, even if it’s not always easy.”
Photo from Unsplash.
Diagnosis is a Light, not a Lamp Shade (Mental Health & IBD Series)
by Aiswarya Asokan (South India)

In front of a grey wall, there is a small green plant in a pot that says "grow grow grow," a table lamp with a white shade and wooden base, and a small moon-shaped nightlight atop a wooden base.
It was on May 2nd 2016, a day before my 19th birthday, for the first time in my life, I heard the word Crohn’s, from my doctor back then. It came as a scientifically valid explanation to all the so-called “sick drama” I was exhibiting through the years. But the excitement of this achievement soon faded away when I came to know that there is no cure for this. Then came the joint family decision, we will keep this diagnosis a secret to ourselves. Anyways, who is going to accept me if they know I have got a disease that makes me run to the toilet and that I have to be on regular medication to stop this from happening. For the next 4 years, I lived like a criminal, fearing for every breath this crime will be caught. In between, I was ill informed about the dietary restrictions I was supposed to follow, and kept eating triggers from time to time, meanwhile wondering why this is happening – but was still focused on keeping the secret safe.
Still, life was a smooth sail with a few days of bad weather here and there, till 2020, when I had my worst nightmare: a serious flare that left me hospitalized for more than 2 months and unable to take my final year university exams. And my secret was out. Not being able to appear for exams was too much for an academically excellent student like me. I was experiencing such intense pain that I couldn’t even turn sides in bed. All this made me question my identity and shattered my fundamental belief system. None of the medicines were working on me. A group of surgeons visited me, and told me that if surgery was attempted, my life might be over on the table. When I realized I might die soon, I decided to live a little. Even though I was not able to eat anything, I ordered a red velvet cake and ate it. The 2020 Tokyo Olympics were going on – it was my all-time wish to watch the Olympics live, but my academic schedule did not allow me to do so. So from the hospital bed, I watched Neeraj Chopra win a gold medal for India, while all my classmates were taking final year exams.
After a while, steroids started working and I started getting better. At the age of 23, I was 33 kilograms, severely malnourished and on a high dose of medication. I was not afraid to die but coming back to normal life was a challenge. I couldn’t face people nor attend phone calls. Even notifications from messages were alarming for me. I zoned out from everyone around me. I felt myself as a complete failure.
One person kept on calling me, despite me ignoring all their calls, until one day I finally picked up. He was my childhood bestie, who stood with me till I was able to manage things on my own. He made a timetable for me, which included slots for physical activity, exam preparations, and fun activities, and made sure I followed them on a daily basis. Then the exam date came up. There were times when I took supplementary exams alone, in a hall that usually accommodates 60 students. Everyday after the exam, he would ask me how it went, and suggest a movie to watch as a reward for the hard work. After a while, exam results came, and I had the highest score than previous years. Life was again on.
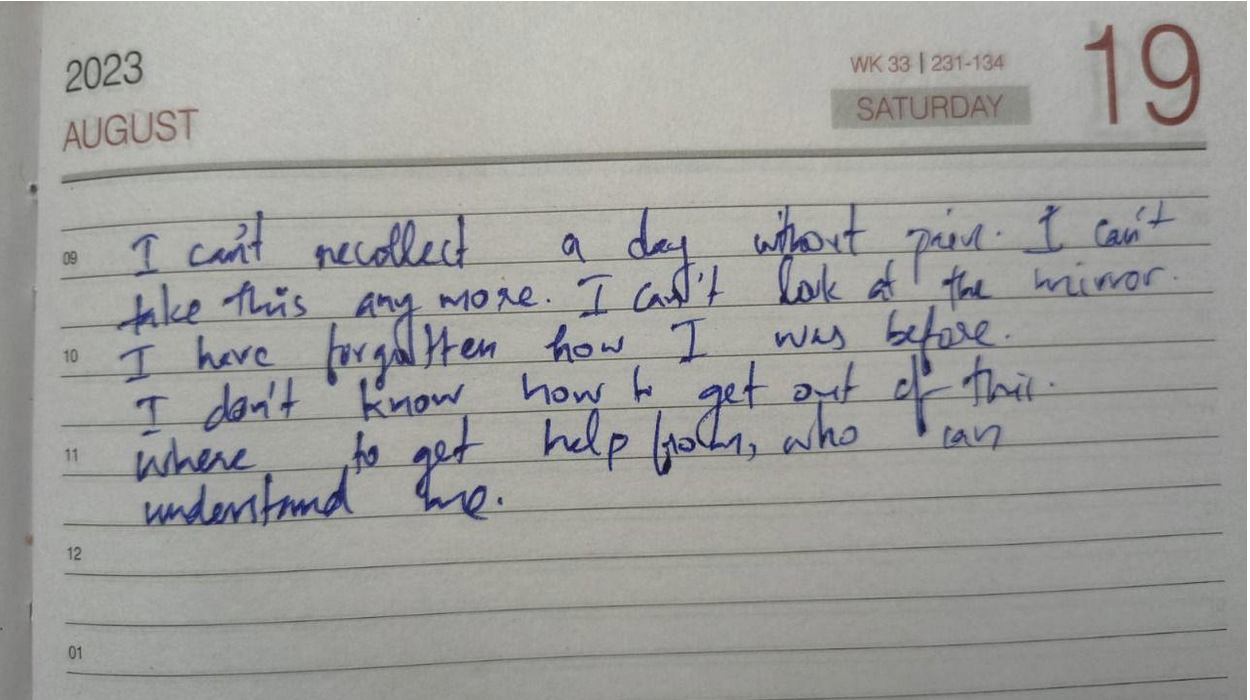
A journal entry from Saturday August 19th, 2023. Text written in blue ink reads “I can’t recollect a day without pain. I can’t take this anymore. I can’t look at the mirror. I have forgotten how I was before. I don’t know how to get out of this. Where to get help from, who can understand me.”
Whenever a flare up hits me, the first thing I notice is a keen desire for physical touch, especially a warm hug, though it sounds strange. I also clench my jaw while asleep, to an extent that my whole face and ears start to hurt the next morning, which further makes it hard to have food. Within the next 3 years, time was up again for a rollercoaster. I had a stricture, unbearable pain, my oral intake was nil, and I had to go for a hemicolectomy. The anticipated complications for the surgery were extremely frightening. This time my boyfriend came up and assured me that “no matter what, I will be there for you.” The surgery went smoothly and I was discharged. I was physically fit but started experiencing PTSD-like symptoms. I started feeling I was just a financial burden to my family.
I slept all day and night as I was not ready to face the thoughts in my head. My boyfriend used to call me every day – just for those few moments I was living, but the rest of the time I used to sleep. This time no friends nor family could help me. Then I started searching for IBD support groups, came to know about IBD India, took the free mental health counselling, and joined the peer group. For the first time, I felt less isolated and felt a sense of belonging. And slowly I replaced my coping mechanism of sleeping with painting. Gradually I was healing, and started feeling more freedom like never before.
Life goes on. Ups and downs are part of it. But when one door closes the other opens. When you feel stuck, ask for help and keep asking until you get one strong enough to pull you out — that is the bravest thing you can do for yourself.
Image from Unsplash.
Mental Health and IBD: An Infographic
by Lexi Hanson (Missouri, U.S.A.)

A light yellow background with pink-orange text reading “mental health and IBD.” There are pink graphics of an intestine and a brain on either side of the text.

A light yellow background with pink-orange text and pink graphics of an intestine and brains. Text included below.
Some connections between Mental Health and IBD (sources included below):
Some evidence supports a reciprocal relationship between mental health and disease activity. Depression is more consistently linked to outcomes than anxiety.
Mental health issues are strongly linked to relapse and recurrence. Stress-related cytokine production likely contributes to inflammation. Anxiety and depression affect treatment adherence, leading to worse outcomes.
Psychiatric comorbidities remain a major driver of poor outcomes and healthcare costs despite advances in treatment.

A light yellow background with pink-orange text and pink graphics of a smiling intestine and brain. Text included below.
Some Daily Habits to Help your Mental Health:
☐ Take medications as prescribed
☐ Eat balanced meals that support your gut health (avoid known triggers)
☐ Drink enough water throughout the day
☐ Practice 5–10 minutes of relaxation (deep breathing, meditation, or gentle stretching)
☐ Check in with yourself emotionally (How am I feeling today?)
☐ Engage in light physical activity if able (walk, yoga, stretching)
☐ Prioritize 7–9 hours of quality sleep
☐ Write down one thing you’re grateful for today

A light yellow background with pink-orange text (included below).
Sources:
Mental Illnesses in Inflammatory Bowel Diseases: mens sana in corpore sano. Bartocci et al. 2023. https://pmc.ncbi.nlm.nih.gov/articles/PMC10145199/
Consensus Statement on Managing Anxiety and Depression in Individuals with Inflammatory Bowel Disease. Hinnant et al. 2025. https://academic.oup.com/ibdjournal/article/31/5/1248/7739104
https://www.crohnscolitisfoundation.org/patientsandcaregivers/mental-health
Listening to Your Body with IBD: The Stoplight System
by Michelle Garber (California, U.S.A.)

A stoplight with red, yellow, and green lights is illuminated on a dark blue night sky.
When you're living with Inflammatory Bowel Disease (IBD), your body becomes its own navigation system. Your body is constantly sending you signals, just like traffic lights do. But unlike the red, yellow, and green lights on the road that we instantly respond to, many of us with IBD have learned to ignore or minimize the "rules" or "drills" that we should follow when our body sends us our own, personal warning signs.
So why is it that we respect a blinking car dashboard, a low battery warning on our electronic devices, and traffic signals/signs more than the signals coming from our own bodies? We wouldn’t ignore our car’s check engine light for weeks (and if we did, we’d expect it to eventually break down). So why do we ignore our body’s warnings? Why don't we listen? As with most things, the answer is complicated.
Here are a few reasons why as people living with IBD, we might forget to listen to these warnings, or try to “push past” them:
Living with IBD means that a few warning lights are always on. That is, we might always have some level of fatigue, bloating, or discomfort. This "always-on" background noise becomes our new normal, and we stop noticing when new signals show up. This is risky because it can lead to ignoring major warning signs or missing slow-building flare-ups.
Our symptoms can become our new normal or "background noise," so we're used to pushing through pain. This means that even when our bodies give us that "red" or "yellow" light signal to slow down or stop due to a symptom/pain that is out of the ordinary, we are still conditioned to push through it. For a lot of us, that is a survival mechanism of having chronic pain (pain that never fully becomes "background noise") in a medical system and society that often tells us to "push through." The world is constructed for those who are able-bodied, and having chronic pain/IBD can force us to sink or swim.
We are often taught to minimize our symptoms, for ourselves and others. Sometimes, doctors dismiss our warning signs, maybe because medical literature doesn't acknowledge all the intricate traffic signals for IBD. Maybe, they're just burned out. Or, maybe doctors—and people in general—can't fully understand the severity of IBD symptoms if they haven't gone through it themselves. Whatever the reason, though, we are conditioned to minimize our symptoms. We are taught that our illness "could be worse." In fact, when explaining IBD to others who don't quite listen closely enough, the false notion that IBD is simply "stomach problems" circulates. So much so that we, ourselves, sometimes say this to others or even believe it ourselves. We don't want to be sick. We wish it was just stomach problems. Being told that our personal traffic lights/signals are simply a result of "anxiety" or "are in our heads" make it easy to eventually believe it ourselves because, why would we want to be sick?
We don’t want to "miss out." Sometimes, we’d rather have a moment of fun—followed by a flare/low-spoons day—than not experience the fun at all. Ignoring the signals can sometimes feel "worth it" since it can give us a small glimpse of what "normal" might be like. We are forever torn between the notions of "respect your body's limits" and "you only live once."
Finding a way to make a choice, despite the consequences, can feel liberating in the short-term. This can look like eating a food that you know isn't "safe" just because you want to make a CHOICE and have autonomy over your own body. As IBD patients, choice is often not in our vocabulary – so pushing through the pain of IBD is often the only way we can feel slightly in control of our own bodies. This is a sense of freedom that we greatly lack as IBD patients.
We don't want to be a “burden.” IBD, in itself, is a burden that we already have to carry. Living with it every day is extremely difficult, and that is an understatement. Even so, we still notice how it affects those around us— our caregivers, partners, family members, friends, co-workers, employers, and even doctors. Carrying the burden alone is never the solution, but it sometimes seems like the right one since it feels wrong to allow someone else to feel even remotely similar to us. It doesn't feel right to allow anyone to be down in the trenches with us—at infusion appointments, at ER visits, at ICU admissions, or at "bathroom sleepovers." It doesn't feel right to allow anyone to feel so wrong, even if they want to. Therefore, we ignore the signs, because if we took action that would mean that we'd need help, whether we like it or not. We'd have to reach out to someone, even if that's just a doctor. Simply alerting your doctor that you've failed another biologic can make you feel like a burden since you might feel as though you're giving them more work. Reaching out to loved ones can be even harder as they will often want to be there for you, and you simply don't want to burden anyone anymore.
We’re afraid of what we’ll find if we stop and really listen. As previously mentioned, we don't want to be sick again. We don't want to discover a new co-morbidity again. We don't want to switch medications again. We don't want to be flaring again. We don't want to go to the hospital again. We don't want to experience medical trauma again. We don't want to put life on pause again. We don't want to miss out again. We don't want to be a burden again. We don't want to lose control again. Listening to your body, and truly paying attention to what it's telling you poses the risk of you having to accept the fact that you might have to go through all of these things again. And at the end of the day, we just want to live—freely. It feels like a constant tug-of-war between surviving and actually living.
The truth is: Your body will always tell you what it needs. It’s just your job to check in—gently and consistently.
Since there is no cure for IBD yet, much of this disease has to do with symptom monitoring and, thus, taking as many preventative measures as possible. I, for one, know that I would like to stay in remission and avoid a flare-up for as long as possible. Even so, I know that's only possible if I listen to my body—genuinely listen. Whether that's taking note of unusual fatigue or nausea, a new sensitivity to food, etc., these are acts of listening to your body and its signals. While we are taught from a young age what traffic lights mean and why it's important to follow them, we aren't taught how to notice and follow the signals that our bodies give us.
A few simple things that you can do to start the practice of ‘checking in’ with yourself and your body:
Create your own ‘traffic light:’ write down some of the signs you notice, when you’re feeling ‘green, yellow, or red!’
Set aside a few minutes each day to ask yourself: What "color" am I today? What makes me that color? What am I feeling, and where am I feeling it? If I’m yellow or red, what needs to change? If I’m green, what can I do to stay there?
Not sure where to start? Here’s an example of my “traffic lights,” and some of the signals I use to check in with myself and my body!


A light blue background with a boarder of green triangles. The text reads “Green means you’re good to go! It doesn’t mean you’re “cured.” With IBD, there’s no one-size-fits-all version of wellness/remission, but it means your body is operating at a manageable and comfortable baseline. When you’re in green, lean into it! Move your body (if you can), make plans, enjoy safe foods, and take note of what helps you stay in this zone. Celebrate ‘green days’ without guilt. They are precious!” There are bullet points with “green light signs” below, the text reads “No Signs of Infection or Illness, Up-to-date on Medications, Overall Mental Clarity, Overall Emotional Stability, Doctor Cleared for Basic Activities, Feeling Energized/Rested, Eating Well-Tolerated Foods, Regular Bowel Movements, Healthy Consistency of Stool, Medications Working Effectively, No Incontinence, No Urgent Bowel Movements, Stable Lab Work, Hydrated, No Constipation, and Minimal Pain/Bloating.” Scattered throughout the page are graphics of a stoplight, a full gas symbol, a fully charged battery, and a green thumbs up."

A light blue background with yellow and black caution tape boarder. The text reads “Yellow is your caution zone. You’re not necessarily flaring, but your body is whispering (or maybe even raising its voice a little). Yellow can be subtle and easy to dismiss, but it’s the most important time to pay attention. In the yellow zone, it’s time to pause and reassess. This may mean: Canceling plans, taking a rest day, eating safe/bland foods, booking a doctor’s appointment, requesting follow-up lab work, reintroducing self-care routines, and more. Yellow isn’t failure. Yellow is wisdom. You’re responding to your body before things worsen. Think of it as preventative maintenance.” There are bullet points with “yellow light signs” below, the text reads “Borderline Lab Results, Mild Changes in Appetite, Changes in Digestion, Low Mood/Increased Anxiety, Sleep Disturbances, Mouth Ulcers, Chronic Nausea, Slight Fatigue/Brain Fog (Not Explained by Medications), Slightly More Frequent/Urgent Bowel Movements, Mild but Persistent Abdominal Discomfort, Decent Consistency of Stool, Mild Joint Pain/Inflammation, Migraines/Headaches, Changes in Skin (Inflammation, Acne, etc.), Worsening Menstrual or Premenstrual Symptoms, or Chronic Bloating.” There are graphics of a yellow stoplight, a half-full gas symbol, a ‘low battery,’ and warning/slow signs.

A light blue background with red EKG patterned boarder. The text reads “Red means something is wrong. It's time to STOP everything else and prioritize your health immediately. This is where IBD forces you to pay attention, whether you’re ready or not. Red means it’s time to: contact your gastroenterologist, take time off school/work, let someone else step in to care for you, follow strict diet/symptom-management protocols, reevaluate or switch medications, get imaging or scopes done, advocate HARD for yourself if you’re not being heard, and go to the ER or urgent care if needed. Red is scary, but it doesn’t mean failure. It means your body is fighting hard and needs you to listen.” There are bullet points with “red light signs” below, the text reads “Ongoing/Sudden Incontinence or Urgent Bowel Movements, Labwork w/ Significant Abnormalities (i.e. Inflammation or Anemia), Complete Loss of Appetite/Ability to Eat, Sudden/Dramatic Weight Loss, Emotional Overwhelm, Not Responding to Medications, Severe Abdominal Pain, Blood in Stool, Mucus in Stool, Dehydration, Fever, Vomiting, or Extreme Fatigue.” There are graphics of a red stoplight, empty fuel tank, ‘stop’ and ‘warning’ signs, and a red low battery symbol.
A few things to remember/keep in mind:
Checking in doesn’t mean obsessing. It simply means being mindful enough to care. Just like we do for our phones, our cars, and our jobs—we deserve to offer ourselves the same level of awareness, support, and maintenance.
Living with IBD doesn’t mean you’ll always be stuck in red or yellow. Some days are green—some weeks or months, even. You deserve to honor those days as much as you manage the hard ones.
This stoplight system isn’t about fear. It’s about empowerment. You are not weak for needing rest, medical support, caregiving, or time. You are wise for knowing when to go, when to slow down, and when to stop.
Your body isn’t the enemy—it’s the messenger. Listen to it. Trust it. Respond with love. Your body is doing the best it can to keep you alive. Let’s return the favor.
Image from @tsvetoslav on Unsplash.
Through
by Michelle Garber (California, U.S.A.)
World IBD Day is May 19th, and this year’s theme is “Breaking Taboos, Talking About It.” Here are 2025 CCYAN Fellow Michelle’s thoughts on stigma, shame, and talking about IBD!
Since being diagnosed with Ulcerative Pancolitis almost four years ago, I have been battling the shame that surrounds my symptoms. I often look back at who I was before my diagnosis—not only grieving that version of myself but also feeling ashamed that I can never fully be her again. Before IBD, I was fiercely independent, reliable, spontaneous, perfectionistic, energetic, athletic, social, focused, happy—and, most importantly, healthy. To put it into perspective: I was a straight-A student at a top magnet school in my district with a 4.44 GPA. I was simultaneously taking college classes, volunteering, traveling, going out with friends, exercising, and serving as the Secretary of my high school’s dance production team. Even during my first year of university—despite COVID-19 restrictions—I took 33 credits, earned leadership positions, made the Dean’s List, got straight A’s, moved into my own apartment, worked out consistently, and started two social work internships.
Then, everything changed. After my diagnosis, my life felt like it had been turned upside down—and in many ways, it had. For a couple of years, I had to move back in with my parents because I could no longer care for myself. There were days that I couldn’t brush my own hair or stand long enough to cook a meal or wash my face. If I needed to go to the hospital, I couldn’t even get myself there. I was fully dependent on my family when my IBD was active. That dependency alone filled me with shame. How could a nineteen-year-old not brush her own hair? How could I be so weak? While I managed to continue online school, I had to request disability accommodations from my university. I went from being someone who never asked for help to someone who needed it in nearly every part of her life. I no longer felt like myself. The woman I once was had seemingly vanished, and in her place was someone I didn’t recognize—someone who carried a constant, heavy shame.
Even now, despite being in remission for about two years, that shame hasn’t disappeared. It creeps in every time I’m too fatigued to answer a text or take a phone call—or worse, when I have to cancel plans. In those moments, I don’t just feel like a bad friend, I feel weak. I feel mentally, physically, and emotionally defeated. I question how someone like me, who seemed to once "do it all," can’t even hold a simple conversation anymore. That shame resurfaces every time I walk into my gastroenterologist’s office or sit in the infusion center waiting room. I think to myself, "Why am I here? I am so young, and yet I am sick. I must just be weak." Even when I pick up a stool collection kit at the lab, I look around, paranoid and embarrassed that someone might know what’s in that big, brown paper bag. I also feel ashamed of what I have to do with that kit once I get home. Especially on the days that I sleep late into the afternoon or feel too exhausted to shower, that shame becomes deafening. I can’t even manage basic self-care, and that makes me feel pathetic and exposed.
Unfortunately, I used to feel as though this shame only deepened when I tried to speak up about what I was going through. On a romantic level, I used to be extremely cautious about sharing my IBD with potential partners. This is because I didn’t want to feel embarrassed, and I certainly didn’t want to be rejected because of it. My first partner after my diagnosis knew all about my IBD. We joked about bathroom "duties" constantly—it was part of our daily rhythm. Beneath the humor, though, I knew that he wanted someone different: someone who could be spontaneous, who could have endless energy, who could cook large meals, who could host frequent gatherings, who could clean, who could work out with him, etc. That just wasn’t me anymore. I also knew that he didn’t want to be around if I ever needed to take Prednisone again since I had explained its emotional toll and side effects. Moreover, I knew that he would "never touch" me if I ever had to get an ostomy. So, I tried to be who he wanted—to become the woman I was before IBD—and for a while, I pulled it off. Over time, though, that relationship made me feel unaccepted—for who I was in that moment and for who I might become. It made me feel ashamed to be me—the real me. It intensified the shame I already carried about my illness.
Since then, dating has been rocky. I’ve met a few people who've responded with deep empathy and genuine interest, and for that, I am grateful. I’ve also encountered individuals who shut down any conversation about IBD out of their own discomfort, who incessantly question my fertility or the "quality" of my genes, or who firmly believe that "tooting" in private or using the word "poo" in a sentence would be impolite and inappropriate. For someone who loves deeply and craves a meaningful romantic connection, those reactions cut deep. They make me question and feel ashamed of the kind of partner I am—or could ever be. On a platonic level, things haven’t been easier. When friends or family joke about me "sleeping all day," "always being at home," "always needing the bathroom," "being forgetful," "not being fun," "eating boring foods," or about how my brother "takes better care" of my dog, shame crashes over me like a wave. I genuinely begin to drown in it. It’s one thing to feel shame for not meeting your own expectations—the ones you set when you were healthy. It’s another to feel shame when romantic partners judge you for something you didn’t even choose and cannot control. However, it’s something entirely different, and perhaps even more painful, to feel that shame reinforced by the people you love and value the most. When they unknowingly echo the same critical thoughts that I already battle every day, it doesn’t just hurt—it reinforces my shame and makes me feel weak and unworthy.
This compoundedness and deeply personal nature of this criticism take my shame and embarrassment to an entirely different level. The intensity of shame I’ve felt in these moments mirrors the shame I’ve carried throughout my journey with active IBD symptoms. It mirrors:
The shame I felt needing my loved ones to brush my hair;
The shame I felt crying, begging, and pleading with doctors for answers and relief;
The shame I felt discussing my symptoms with countless medical professionals;
The shame I felt from the burn marks and scars left behind by overusing a heating pad;
The shame I felt experiencing fecal incontinence;
The shame I felt wearing diapers for months;
The shame I felt needing to carry baby wipes, toilet paper, and a change of clothes;
The shame I felt when I could no longer clean myself without help;
The shame I felt asking my gastroenterologist to remove my colon;
The shame I felt when I began to question if life was even worth living;
The shame I felt being bedridden, needing a wheelchair just to get fresh air;
The shame I felt requesting accommodations from my university;
The shame I felt when a doctor asked me why I waited so long to seek help.
Still, I continue to grieve the version of myself I once was, and I wrestle with the shame of not being able to live up to that image again. Feeling stuck in your own body when your mind wants to do so much more is an agonizing experience. I acknowledge that fully. Yet—despite my doubts—those feelings of shame began to fade away as my symptoms have lessened and as I’ve found my voice within the IBD community. I've recently been able to feel pride when comparing the person I once was to the person I am today. No, I may never again be the energetic, healthy "yes woman" I once was. Nevertheless, I wouldn’t have the resilience, empathy, and sense of purpose I now carry if not for IBD. Fighting for your life, navigating a new reality, and battling stigma while the world moves on without you teaches you something profound: you are capable of surviving the unimaginable.
With this new revelation and mindset, I've come to see how my feelings of shame and beliefs of being weak/perceived as weak are rooted in fallacy because:
To cry in front of doctors and explain your symptoms is not shameful—that's strength.
To be vulnerable and advocate for yourself is not shameful—that's courage.
To decline a call, cancel plans, say "no," and set boundaries is not shameful—that's self-respect.
To rest rather than push through the pain is not shameful—that's self-love.
To wear diapers and pack supplies to manage your day is not shameful—that's determination.
To request or actually go through a life-altering surgery is not shameful—that's bravery.
To need and/or ask for help is not shameful—that's survival.
To live in a body that is constantly fighting against you is not shameful—that's perseverance.
To choose life every day, despite IBD's messiness and pain, is not shameful—that's resilience.
Furthermore, I believe with all my heart that talking openly about IBD—the good, the bad, and the ugly—is one of the greatest testaments of one's strength. Whether it's with friends, partners, family, co-workers, medical providers, or strangers, it takes immense courage to be that vulnerable. This is because, in all honesty, there is risk involved. As human beings, our minds can sometimes jump to the worst possible outcomes. When it comes to talking about IBD, there's the risk of being judged, pitied, and misunderstood. There's the risk of "becoming" your diagnosis and of losing relationships or job opportunities due to stigma. These fears are real and valid, and they’re exactly why many IBD patients tread lightly when sharing their stories. As a result, though, we often overlook the best possible outcomes. From experience, I know that talking about your IBD can: help you feel more at home in your own body; help you feel accepted for who you truly are rather than who people want you to be; help you find community; help shine a light on the genuine/empathetic people in your life; help create space in your mind for something more than just survival; help break the stigma; and help pave the way for earlier diagnoses, better treatments, and stronger support systems. Sharing your story doesn’t make you less—it makes you more. Sharing your story makes you more human, more whole, and more you than you had ever thought possible.
Taking all of this into account, I’ve come to recognize how powerful it can be to talk about IBD and share your story. If the worst that can happen is being judged, excluded, misunderstood, or left, then maybe talking about your IBD is a blessing in disguise. I know that speaking openly about my IBD has saved me from dedicating my energy and love to people who didn’t deserve it. If the best that can happen is finding your people, becoming more comfortable with your diagnosis and yourself, getting care faster, and helping to break the stigma, then sharing your story might actually be a superpower. We, as IBD patients, are in a unique position to educate and advocate—not because it’s our responsibility, but because our lived experiences often speak louder than medical textbooks ever could. I wish we lived in a world where everyone understood IBD, where institutions offered protection, and where systems were built to accommodate us. The truth is, though, most people just don’t know where to start. They rely on what they read online or hear in passing. It’s easy to see how misconceptions and stigma grow. If I read online that remission meant "no symptoms and a healthy colon," I probably also wouldn’t have much empathy for someone in remission who still canceled plans or needed extra rest. As someone in remission who is sharing her story, though, I can tell you one thing: that version of the story isn’t quite right. Nothing about IBD is so black-and-white. Everyone’s experience is different, which is why personal storytelling matters so much. Doctors, loved ones, and even other patients learn from us as IBD patients. So many vital conversations—about non-textbook flare symptoms, about “safe foods,” about unspoken medication side effects, and about what remission really looks like—don’t come from medical journals; they come from people with IBD who tell the truth about what it’s actually like. Without these stories, diagnosis and treatment can be delayed, and support systems stay broken. It’s not our job to fix the system, but by speaking up, we might just make it easier for those who come after us. We might even make it easier for ourselves in the future.
For a disease that has made me feel powerless more times than I can count, finding power with or over my diagnosis has been invaluable. Talking about IBD has helped me reclaim my own narrative. People can still judge me, but at least they’re judging something real. If someone can’t handle a story of resilience, that’s on them. No journey of survival is without its dark moments. Most movements worth remembering were forged in hardship.
That said, I don’t want to pretend it’s easy. Even now, I still struggle to talk about my IBD. I just recently began experiencing symptoms of a flare, but I only told my doctor and loved ones after a delay. This was not out of embarrassment, but out of fear—the fear of returning to that time when I felt that I had lost all independence, the fear of being blamed, and the fear of blaming myself. There’s a voice in the back of my mind that whispers, "You should’ve taken better care of yourself. You should've been stronger." And although I know that’s not true, it still stings.
Even with that fear, though, I eventually reached out because I’ve learned what happens when I don’t. I know now that silence doesn’t save me. Hiding doesn’t protect me. Every time I have tried to ignore a symptom or push through for someone else’s comfort, I’ve paid for it tenfold. I've realized that delaying diagnosis and treatment is, quite frankly, not worth anything. So, I’ve started doing the hard thing: I've started telling the truth. I’d rather speak up than wait until things become unmanageable because the truth is, IBD is messy. It’s not just a bathroom disease. It’s not just about inflammation or test results. It’s about what it does to your relationships, your identity, and your sense of safety in your own skin. It’s about mourning the life you thought you would have, and then figuring out how to build a new one—without pretending that the old one didn’t matter. It’s also about power—quiet power. This is the kind of power you reclaim when you speak up, when you stop hiding, and when you say, "Here’s what I’m going through," even if your voice shakes.
I know what it’s like to walk into a doctor’s office, share your story, and be dismissed. I know what it’s like to be lonely in a room full of people who love you. I know how scary it can be to share what you're going through. At the same time, I also know how healing it can be. Talking about your IBD—when you’re ready—can give you strength with the diagnosis and over the stigma. That kind of power is slow and sacred. It doesn’t always feel good, but it builds something stronger than "perfection" and "control." It builds truth. When I tell my story, I don’t just feel more seen. I also make space for other people to show up with their stories. Sometimes, your courage can be the reason someone else finds theirs and feels less ashamed. The more we speak, the less shame survives. The more we share the parts of IBD that don’t have tidy endings, the more human this disease becomes rather than being a punchline of a joke or a pity project. There are days that I still feel afraid—afraid of being judged, misunderstood, and left behind. Even so, I’m more afraid of going through this alone. If my story can be a hand reaching out to someone else in the dark, then I’ll keep telling it—again and again. At the end of the day, I truly believe that the only way out is through, and for me, the "through" begins with sharing my story.
Flare-up: A Downward Spiral
by Akhil Shridhar (Bengaluru, India)

A black and white image of a spiral staircase (view from above).
It all begins with a flare-up. For most of us, the diagnosis comes only after enduring symptoms for days or months, dismissed as a stomach bug. But when the discomfort escalates into a significant disruption, we hear the term “flare-up” for the first time. The symptoms build like a chain reaction, growing worse until urgent medications—usually steroids or antibiotics—are prescribed for relief.
Difficulty with Food
Almost every food item can trigger nausea or an urgent trip to the restroom, making nutrition a frustrating challenge. While some believe short-term food restrictions might ease inflammation, prolonged deprivation causes more harm. In countries like India, navigating diverse dietary recommendations complicates matters. As newly diagnosed individuals we often seek advice in support groups, hoping for recipes or meal plans that won’t worsen symptoms. But in most households, skipping meals isn’t acceptable. Our parents insist on “good food,” unaware that their concern often fuels the next domino.
The Washroom Runs
Initially, the frequent restroom trips are an inconvenience—but soon, they dictate life. The unpredictability makes outings stressful, and hesitation around food becomes constant. Exhaustion follows, leaving us dehydrated, fatigued, and mentally drained. The cycle feeds itself: eating triggers symptoms, symptoms disrupt daily activities, and fatigue makes even basic tasks overwhelming.
The Mental Toll
Beyond the physical struggle, IBD takes an emotional toll. The anxiety of unpredictability, the frustration of adapting to a condition that doesn’t follow rules, and the isolation of feeling misunderstood weigh heavily. Conversations become filtered—friends may not fully grasp the challenges, and outings are haunted by the fear of urgently needing a restroom.
Sleep Struggles
IBD doesn’t stop at meals—it disrupts rest too. Pain, restroom trips, and anxiety make sleep elusive, worsening inflammation and fatigue. Poor rest perpetuates the cycle, making daily recovery harder. Many of us try strict bedtime routines, meal adjustments, or sleep aids to reclaim rest. While perfect sleep remains rare, small efforts help ensure the limited hours of sleep offer some recovery.
Finding Balance
What I have realised after a few misadventures is that the best way to get out of this spiral is to consult your medical team and get the required medications right away. The damage that prolonged inflammation has is quite severe and takes months if not years to reverse, sometimes is unfortunately irreversible, therefore it is not worth the risk of ignoring it.
IBD is unpredictable and exhausting, but it doesn’t define life. Over time, we find dietary adjustments, support systems, and coping mechanisms to regain control. Gradually, these adjustments help restore control—accepting the hard days, seeking support, and celebrating small victories. While flare-ups will always come and go, so does recovery. Life continues, not perfectly, but uniquely. And within that cycle, resilience proves stronger than the condition itself.
Image from meister_photos on Unsplash.