

NEWS
IBD and Eating Disorders: Control, Fear, and Survival
by Michelle Garber (California, U.S.A.)

An empty pink-orange plate with a knife and fork on a white background. The plate and utensils have some food remnants left on them, as though they were recently used.
Content Warning: this article discusses eating disorders and topics such as food restriction, binge eating, and body dysmorphia.
For as long as I can remember, food has never been just food. It has been comfort, control, fear, shame, and even the sole measure of my worth. I began struggling with disordered eating as a child, long before I knew anything about Inflammatory Bowel Disease (IBD) or ulcerative colitis—the chronic illness that would later reshape my relationship with my body all over again.
My earliest battle was with anorexia nervosa. I was only around twelve when I began restricting food, counting every calorie, and chasing the illusion of control that came with watching the number on the scale drop. Almost no one knew. The secrecy was part of the sickness—the quiet shame that thrived in silence. It felt safer that way. In a strange way, that shame felt familiar when I was later diagnosed with IBD. Both conditions carried a stigma. Anorexia was whispered about in terms of vanity and control, and conversations about IBD were avoided altogether because they involved the "uncomfortable" topics of bowels, bathrooms, and bodies.
By my senior year of high school, I had relapsed in terms of my anorexia. With prom and graduation approaching, I wanted to "feel confident" in my own skin, but my desire for control quickly turned into obsession again. I convinced myself that going vegan and gluten-free would "clear my acne" and "make me healthier." When it didn't, though, I continued anyway. I continued because I had found something else: the rush of watching the scale drop again. I told myself that it was about health, but deep down, it was about control, perfection, and fear.
When COVID hit, prom and graduation vanished, but my eating disorder didn't. Even though I eventually abandoned the vegan diet, my restriction continued. My hair began falling out in clumps. I was so weak that I needed to be pushed in a wheelchair on family walks and through grocery store aisles. Still, I clung to denial, blaming my fatigue and hair loss on my thyroid. I wasn't ready to admit that I was sick again—not from a medical condition, but from the same mental illness I thought I had conquered.
The human body can only endure starvation for so long before it rebels. Mine did—violently. The pendulum swung from restriction to bingeing. Binge eating disorder involves recurring episodes of eating large amounts of food rapidly, often to the point of physical discomfort, accompanied by feelings of loss of control and guilt afterward.
That was my reality. I gained weight rapidly and felt completely out of control. If anorexia gave me a false sense of control over my life, binge eating disorder stripped it away. I swung from one extreme to another, and both made me miserable. When the weight gain triggered the same familiar self-loathing, I spiraled right back into an anorexia relapse again—a vicious cycle of control and chaos that consumed years of my life.
Eventually, my body began to fail. My heart rate slowed to dangerously low levels. For the first time, I allowed myself to admit the truth: I did not want to die. Recovery, for me, began not with love for my body, but with the simple desire to stay alive.
I began eating again, slowly and carefully. On paper, it looked like recovery—my calories were adequate and my body was functioning. Mentally, though, I was still trapped. I measured every ounce of food, logged every calorie, and spent hours preparing meals to ensure perfect precision. I told myself that it was about maintaining my metabolism, but it was still about fear—the fear of losing control, the fear of gaining weight, and the fear of trusting my body.
Even when I was "eating normally," my life revolved around food. I avoided restaurants unless they posted nutrition information online. I sometimes ordered takeout, only to bring it home and weigh it myself. I had simply traded starvation for obsession. I thought that I had my eating disorder under control, but in truth, it still controlled me.
Around this time, I began experiencing digestive symptoms: constipation, vomiting, reflux, and pain. I now believe that my disordered eating—the pendulum swing from restriction to bingeing, my extremely high insoluble fiber intake in order to eat high volumes of food with the least amount of calories, and my reliance on laxatives due to my food restriction—played a role in triggering my ulcerative colitis, along with the mental/emotional stress caused by it all.
When I was finally diagnosed with IBD, I thought that my disordered eating would take a back seat. I was wrong. Chronic illness can be fertile ground for eating disorders to grow. The constant focus on diet, the fear of flares, and the unpredictability of symptoms can reawaken old patterns of control and restriction.
In the hospital, I was prescribed prednisone and given a list of "safe foods." Back home, I stuck to that list religiously. Underneath it all, though, my old compulsions still resurfaced. I limited not just insoluble fiber, spicy foods, dairy, and alcohol—which are common triggers during flares—but also carbs, sugars, and sodium. This was due to the fear of prednisone-induced weight gain—the water retention, "water weight," or "moon face" that prednisone could cause. I told others that it was about inflammation, but in truth, I was relapsing again—this time under the socially acceptable cover of a "medical diet."
This is one of the hardest truths about eating disorders and IBD: the overlap between medical management and disordered eating behaviors is often blurred. The two can feed each other in quiet, dangerous ways.
IBD can create new patterns of disordered thinking in people who have never struggled with eating disorders before. This is because when your body betrays you like it does with IBD, food becomes (or at least feels like) one of the few things that you actually can control. Plus, when your weight fluctuates rapidly—sometimes losing as much as thirty pounds in a week and then regaining it soon after—it can completely destabilize your sense of self.
For those with body dysmorphia or a history of disordered eating/anorexia, this is especially dangerous. There's no such thing as "small enough" in the mind of someone with an eating disorder. Seeing a "low" number on the scale (even when it's caused by illness) can increase your dopamine and ignite the urge to chase that number, again and again. I remember logically understanding that my low weight during my flare was unhealthy, but emotionally, I still felt anger and panic when the scale went up after treatment. Prednisone's mood swings certainly didn't help with this either—I was at war with both my mind and body.
Now, in remission from IBD, I can finally say that I am also in recovery from my eating disorders. Even so, recovery (like remission) is never as simple as it sounds.
Even in remission, disordered eating behaviors can quietly persist. For many of us with IBD, it shows up as hypervigilance around food: the fear of new foods, the obsession with "safe" meals, or the guilt after eating something "off-plan." It can look like avoiding social events involving food, fixating on weight fluctuations caused by steroids, or tying self-worth to whether symptoms worsen after a meal. These behaviors can masquerade as "caution," but they're often echoes of deeper fear—the fear of pain, the fear of loss of control, and the fear of being sick again.
The parallels between IBD and eating disorders are striking. Both involve an uneasy relationship with the body—a sense that your own physical self has turned against you. Both can make you feel powerless, trapped, ashamed, and isolated. Both can lead to cycles of control and surrender, as well as perfectionism and self-punishment. And both are often invisible to others, hidden behind a mask of composure and "doing fine."
Today, my relationship with food is no longer about control—or at least, I'm trying to keep it that way. I eat intuitively when I can, forgive myself when I can't, and I remind myself that nourishment is not a punishment or reward; it's an act of care. My body has been through battles most people can't see—battles maybe I never even noticed. My body deserves gentleness, not control or being told that it isn't "good enough." Yes, my body may have not been the kindest to me over the years, but I also haven't been the kindest to it in return. While my body may have betrayed me in some ways due to my IBD, it has also gotten me through my IBD, my eating disorders, and so much more. My body is not my enemy. My IBD is not my enemy. My weight is not my enemy. How I look in the mirror one day versus how I look in the mirror the next is not my enemy.
Living with both IBD and a history of eating disorders means constantly walking the line between vigilance and obsession, as well as between self-protection and self-harm. Even so, I've learned that healing is not about never struggling again—it's about recognizing when the struggle starts to whisper and, this time, choosing to listen with compassion instead of control.
For more information on disordered eating & IBD, check out this patient-created resource by the ImproveCareNow Patient Advisory Council.
Image from @jogaway on Unsplash.
My Complicated Relationship with Food
by Kaitlyn Niznik (New York, U.S.A.)

Artwork by Kaitlyn, titled “Taste the Rainbow.” The background is bright teal with an out-of-focus rainbow. Overlaid are drawings of brightly colored fruits and vegetables, including an avocado, grapes, a peach slice, pomegranate seeds, blackberries, asparagus, corn, strawberry, banana slice, blueberries, broccoli, carrot, raspberries, yellow bell pepper, peas, beans, and thinly sliced cabbage.
When I first showed symptoms of something wrong, I blamed food poisoning or bad college campus food. I stuck with these excuses as I left undergrad and started grad school. Granted, my grad school food was horrible during my first residency - I will never look at squash lasagna the same way again. However, when I came home and got even sicker, I knew I needed to get checked out. Since then, I've seen four gastroenterologists and a nutritionist - each one with their own advice regarding food. Some of the advice I was given include: become a vegetarian, eat low FODMAP, low fiber, low roughage, low gluten, stick to soups/stews, just eat homemade food, switch over to the brat diet on bad days. I'm someone who was never consistent enough to try a true elimination diet and all the diet restrictions became overwhelming. With my long hours at work, I didn't have a ton of free time or energy to meal prep everything and I got discouraged when my homemade food still made my symptoms flare up. After four years of trial and error, here are three things that are helping me develop a healthier relationship with food:
Hydrogen Breath Tests
Breath Tests are non-invasive tests that gave me insight into my food intolerances. They're more specific than just banning all FODMAPs and if you know what to avoid, it's easier to figure out portions and safe amounts. I found out I have a fructose intolerance, so I eat fruits and vegetables in moderation and avoid high fructose corn syrup.

Artwork by Kaitlyn, depicting a hydrogen breath test. A purple bag with a nozzle to blow into sits beside a cup filled halfway with liquid. The background is bright teal.
Biodiversity in Bites
I try to graze on fruits and vegetables whenever I pass by the kitchen. With my fructose intolerance, I can't eat a lot of fruits in one sitting, so I try to spread out little amounts throughout the day. Even if it's a frozen quarter of a peach, half a banana, or a few steamed baby carrots, every little bit helps promote biodiversity in the gut. Before, I was so focused on meeting the daily recommended portions of fruits and vegetables that I became disheartened whenever I failed to reach that goal. Nowadays, I aim for a bite of a few different fruits and vegetables at meals and throughout the day. To make it happen, I steam or bake vegetables and then put them in the freezer in bags so they're easy to break up. I can easily take a handful of black beans and corn for a quesadilla or parsnips, celery, and carrots for a soup. I am happy to say this is my first fall making stewed apples and it's now become a staple to meal prep each week! Stewed apples are easier on my stomach and are packed with soluble fiber. I have also combined them with cranberries to make cranberry apple sauce that's rich in vitamin C. I'm happy I can find ways to enjoy the flavors of fall without the stomachaches.

Artwork by Kaitlyn, titled “Taste the Rainbow.” The background is bright teal with an out-of-focus rainbow. Overlaid are drawings of brightly colored fruits and vegetables, including an avocado, grapes, a peach slice, pomegranate seeds, blackberries, asparagus, corn, strawberry, banana slice, blueberries, broccoli, carrot, raspberries, yellow bell pepper, peas, beans, and thinly sliced cabbage.
“Human kibble"
Thank you to tiktok user @myfoodisme2 because this is my new favorite meal prep obsession. Before, I felt so limited eating only soups and some weeks it felt like too much work to create balanced and delicious meals. Human kibble is essentially a basic formula for a quick bowl with a lot of diversity. It’s like a Buddha bowl, but less artfully arranged and more thrown together. This is the formula I’m using for meal prep:
Base (Rice/couscous/quinoa) + Protein (Chicken, tofu, beef) + Veg (A little of everything)
For me, a spoonful of beans is safe, as is a bite of cooked broccoli, corn, carrots, etc. I think of it as a nutrient-dense mix that has streamlined my meal prep. Each component can be prepped separately and then combined in the fridge. Unlike portioning giant stir-fries where I have no idea how much of each ingredient I'm getting in a single bowl, I can combine the ingredients right in my lunch containers so I know exactly what I'm eating each day. It's much easier to see patterns or know what gave you a stomach ache when you're keeping things consistent and just tweaking a basic formula each day.

Artwork by Kaitlyn, depicting a dark teal bowl with a variety of ingredients, such as tofu, broccoli, peas, beans, carrots, and grains. The background is bright teal.
Artwork by Kaitlyn Niznik!
Revolution in Diet Therapy for Inflammatory Bowel Disease: A distilled summary
A Summary of Revolution in diet therapy for inflammatory bowel disease - Melton - 2024 - JGH Open - Wiley Online Library
By Peter Park, Plano Texas

Disclaimer: This piece is not intended to serve as medical advice, but as a reflection on strategies for patient advocacy. Always talk to your GI provider before making any changes to your diet, medication regimen, or any other aspects of your health care.
This is a review article that compiles several studies which center around how diet interplays with Crohn's disease and colitis. Articles are subcategorized by well known factors that contribute to inflammation including meat, dairy, additives, and fiber. Articles and studies are also graded on academic rigor with the gold standard being a randomized control trial and lower quality studies being observational data.
Exclusive Enteral Nutrition (EEN)
First, the article talks about EEN. What is EEN? EEN stands for Exclusive Enteral Nutrition, which means nutritional resources come from a liquid formula for 6-8 weeks (gross). EEN has been shown to achieve clinical remission similar to corticosteroids in pediatric populations. Adult populations seem to follow a similar trend.
Compared to steroids, using a EEN liquid formula based diet is way better to remove the potential harmful side effects of steroids. More specific data shows that factors such as male sex, younger age, milder disease, and certain microbiome profiles respond better to EEN. One criticism can be the healthy user bias where study participants are naturally going to be healthier people and that the person who can tolerate EEN for 6-8 weeks may just be a more self-disciplined person with less financial or social barriers, and overall healthier person.
Partial Enteral Nutrition (PEN)
Let’s be real. Would you sign up for a smoothie-only diet for 6-8 weeks? Authors looked into other diet options such as PEN or Partial Enteral Nutrition where only a portion of food intake is liquid formula and the rest is unrestricted food intake. However, studies have not been promising in PEN’s ability to reduce inflammatory markers such as fecal calprotectin or CRP. Whether that's because of poor ability to stay on that diet or whether that's because of the diet itself is hard to say.
Crohn’s Disease Exclusion Diet (CDED)
Crohn’s Disease Exclusion Diet (CDED) uses 50% PEN and permits only certain foods in three phases:
Phase 1 - Chicken breast, fish, lean meats, olive oil, onion, potatoes, rice, tomatoes
Phase 2 - certain legumes, fruits (blueberries, kiwis, and peaches), vegetables (broccoli, cauliflower, sweet potato, and zucchini), oats, whole-grain bread and pasta
Phase 3 - can introduce foods such as alcohol, coffee, dairy, grains, and seafood
Foods to avoid in ALL phases - Process meat, artificial sweeteners, seeds, emulsifiers, and preservatives
CDED has been shown to reduce inflammatory markers but has yet to be validated in a larger scale study.
Find more information about the Crohn’s Disease Exclusion Diet on the Nutrition Therapy for IBD website.
Diets for Ulcerative Colitis
There's exciting new evidence in ulcerative colitis that indicates that high levels of Hydrogen sulfide (H2S) can increase disruption of the microbiome and cause injury to the colon. Fecal transplant has also been shown to be more impressive and impactful in reducing inflammatory markers when paired with a plant based and low protein based diet. The Mediterranean diet has also shown to improve inflammatory markers but it still seems unsure whether the Mediterranean diet alone is causing this or whether it's the removal of the standard American diet which is known to be high in fats and protein.
I personally want to focus not on any specific diet but the overarching data that seems to indicate that avoiding processed foods, especially processed meats, can help to reduce inflammatory markers. Whether that reduces symptoms from a subjective patient point of view is a little harder to capture in the data. So far, the evidence is clear: There is no evidence that IBD can be treated with diet alone.
Our disease as IBD patients is still a medical disease that requires specific medications and Hopefully we can continue to see more diet and nutritional studies as we all have personal common-sense-knowledge that diet does impact our flares.
One of the best ways to personalize your own flares is to capture a food journal where you can document certain food triggers that occur with flares. This can be really useful in bringing to your gastroenterologist or other specialist, in order to develop a diet plan that works for you. There’s real hope in using food as part of your treatment plan, and with the right approach, it could help you feel more in control of your IBD.
Featured photo by Dana Tentis from Pexels.
A Not So Invisible Illness: Inflammatory Bowel Disease
By Maria Mutka from NC, USA

Content Warning: Body dysmorphia, abnormal eating and exercise patters.
As a high school teenager, I thought I was doing well at hiding my illness from my friends and peers. When there were snacks or meals served at school that I knew would send me straight to the bathroom, I deftly avoided them and made excuses that I had already eaten or just wasn’t hungry. If I was experiencing extreme abdominal pain, bloating, and gas during the school day, I tried to ignore it while positioning myself as close to the door as possible, just in case.
For most of high school, I experienced a constant flare that fluctuated between mild and moderate symptoms. This made hiding the tangible symptoms of my ulcerative colitis somewhat possible in my mind, although my friends and peers undoubtedly knew I was experiencing gastrointestinal health issues. I had briefly mentioned to them before that I had inflammatory bowel disease (IBD), but avoided elaborating on what that meant out of embarrassment and fear that it would make them uncomfortable.
I soon realized that there was one facet of my illness I could not hide from my classmates: while being a sophomore in high school, I was 5’2” and barely 80 lbs., with the face and the body of an 11- or 12-year-old. This visible manifestation of my illness through delayed puberty caused me to experience a lot of insecurity, which in turn led to becoming obsessed with food intake and exercise. I was constantly trying to find the perfect balance between food and exercise that could overcome the deleterious impacts of my ulcerative colitis on the absorption of nutrients critical to my growth.
Perhaps the reality of my underdeveloped body so heavily impacted me because of my journey with ulcerative colitis since the age of 6. I had gotten used to the other physical manifestations of the disease: frequent bowel movements, diarrhea, blood, pain, and extreme fatigue, but this limbo stage of early pubescence was new to me. It was extremely damaging to my adolescent attempts at processing and accepting my body for what it was, and at developing anything resembling a positive body image.
At the time, it felt as though with my IBD symptoms continuing, the very least my body could offer me was a sense of somatic belonging and self-worth that I felt could only come from looking like my peers. I was determined that looking my age would help me finally feel like I had access to the same sort of normal teenage experiences they did. Maybe once I looked like everyone else, I would feel more confident in making new friends, being involved in athletics, straying outside the comfort of a singular, perfectionistic focus on academic success by making mistakes, and dating.
For so long, I let my physical appearance dominate my social interactions and extracurricular activities because I felt like an imposter in my own body, completely estranged from what I thought it meant to be a teenager like my peers. In my mind, I was only able to watch from the sidelines as high school, along with the seminal memories and lessons that accompany adolescence, unfolded for everyone else.
Part of the issue was that I was not simply imagining my peers’ perceptions of my physical appearance. Under the guise of concern, while trying on costumes for high school theater productions, several of my peers would tell me that I needed to eat more, bluntly stating that I looked like a twig. In those moments, I could not have felt more infantilized or more childlike not only in appearance but in how my peers treated me.
It was not only my peers who infantilized me. Eventually, I was referred to an endocrinologist for my stalled growth. While I had looked forward to identifying possible solutions to my inability to gain weight and progress further in puberty, all I received from my doctor were vague assurances I would eventually grow and that my endocrine system was in working order. These small efforts at placating the concerns that were wreaking havoc on my mental and social quality of life while well-meaning, were harmful. They reinforced my ever-growing anxiety that my situation would never change and that my mental health and social quality of life did not matter.
My experience with US health care systems’ large deficits in addressing chronically ill youths’ psychosocial needs and quality of life is, unfortunately, not at all unique. Whether these needs are avoided intentionally through health systems causing direct medical trauma, or through omission in failing to address social determinants of health (e.g., housing needs or food needs), the harm done is impactful and lasting. If providers had screened for or discussed my mental health and psychosocial needs related to my IBD at any point, I would have jumped at the chance to talk about it. However, my physical symptoms were the only topic of discussion and implied to be the only issue that could even concern me.
I know now that delayed puberty is not an uncommon comorbidity of pediatric inflammatory bowel disease, as many studies on the subject have shown. Despite my at-the-time unassuageable fears, I did eventually grow and complete puberty, although I do still receive comments that I look young for my age.
Looking back at my adolescence, when I felt like I was perpetually stuck in a Groundhog Day scenario due to my delayed puberty, in hindsight, I can appreciate all my body did for me. I was able to make it through a multi-year-long flare, and all things considered, my body managed it pretty well. Looking back, I try to have compassion for my perfectionistic teenage self who was determined to look like her peers to an unhealthy extreme. What she needed was a pat on the head or vague assurances everything would turn out okay. She did not even need hormone therapy, medication, or any sort of quick fix to help her start puberty earlier. It was in many ways a lot simpler than that: she needed providers and a broader health care system that could recognize her need for mental health support and do something about it.
Featured photo by mododeolhar from Pexels.
It's not all about the bass - feeling comfortable in your skin.
By Maalvika Bhuvansunder

Ahh, the ever classic “All about that bass”, the so-called “revolutionary” song which was meant to show body positivity. One question though: How is it body positivity if you are putting down other body types? Body shaming is something I have endured constantly. Growing up, I was an extremely plump and chubby kid. Every vacation used to be a nightmare with relatives constantly telling me to eat less and become slim. To a preteen! That's where the root of my low self-esteem began. I was told by people that I wouldn't have friends if I don’t reduce weight. So growing up, when I did not understand the lyrics, it's all about that bass… by Meghan Trainor was a revolutionary song for me. It made me, and I’m sure a lot of other girls like me, feel amazing about our bodies. But what about the others?!
I was told by people that I wouldn't have friends if I don’t reduce weight.
A few months before I got my diagnosis, I started losing a lot of weight. Each month I would have lost around 2-3 kgs. Very soon, the chubby girl became the skinny one. It was very confusing for me and my parents as to why I was losing all this weight. Post the diagnosis, at least we knew the reason. It was very new and weird for me to look this thin and I knew this was not a healthy weight loss, but I did not have any control over it. Keeping down food got difficult, and I developed this fear of eating as it was associated with pain. What added to this were the comments of other people.
There was one group that cheered this weight loss, glorifying it without knowing the pain I was in. Then, there were the others that made me feel ashamed of being so skinny. The constant, why don't you eat, are you trying to diet, you looking this skinny is UGLY got too much. I refused to step out of my house because of this constant judgement. Random strangers used to advise me on how to gain weight and that being this skinny is not good. Strangers did not know the cause of my weight loss, but when the family and friends that did know about it made such comments, it hurt the most. The constant comparison with others in my family to casually making “jokes” and trying to funny about my weight was horrible for me. It was impossible for me to gain any weight, and it was not like I did not know that I was dangerously underweight. But “Eat up!” was not the solution, and food was the main pain-causing component for me at that time.
If you are healthy and feel great, then who cares what shape and size your body is? People are going to comment either way.
Post-surgery, now that I am able to slowly gain weight, this fear is always still there of what if I go back to my preteen body type. On the other side, the fear of relapse in weight gain is also there. I’m sure a lot of individuals with IBD would experience body dysphoria, the feeling of not belonging in your skin, and hating the way you looked in the mirror. That was me for most of my life. This experience made me realize that what truly matters is feeling healthy. If you are healthy and feel great, then who cares what shape and size your body is? People are going to comment either way. What truly matters is your health. To this date, I am not fully comfortable in my skin, but I am making baby-step progress towards it.

What I Eat in a Day
TW: mention of eating disorders & disordered eating
I really didn’t want to write this article. I am pretty open about how I have a lot of dietary restrictions. When I go out to eat with friends, I usually tell them that I follow a strict diet for my Crohn’s Disease. Then they’ll ask if I can have anything on the menu, and I will say No. The inevitable next question is always: So, what can you eat? I’ll list off a few foods like oats, bananas, blueberries, broccoli, chicken, and buckwheat, and that's usually the end of that conversation. I’ve had it so many times; honestly pretty much any time I meet somebody new.
I tend to think that when I give people that list that they just assume I stop listing things because it would get excessive if I named every food I could eat. I imagine that they might think I am going through a typical day, and maybe other days look different than the short food record I have given. I don’t think that anybody really considers what it feels like to eat the same 5-10 foods over and over and over and over again. But I do. I do because that has been my life since January of 2019 when I entered “remission”.
Remission for me has always been rocky. I noticed really quickly that while I felt better overall (you know, my body wasn’t trying to set records for lowest hemoglobin and highest CRP simultaneously), I still had some symptoms. I decided to take the advice I give a lot of my IBD patients these days and start a food journal to try to find my trigger foods. Slowly I started feeling better as I cut back on the foods that I noticed were giving me hives, acne, bowel cramps, diarrhea, and a whole host of other symptoms.
So I got to a baseline diet with some foods I knew I felt good on and did that for a bit. It was wonderful, as long as I ate these foods, I felt pretty much “normal” and could do all the activities I wanted. But I wanted to find more things I could eat, so I started to do food reintroduction. I would try a new food for one meal and see how I felt afterwards. If I felt worse, I knew that food wasn’t a good fit and I’d mark it as a trigger food.
Fast forward to 2+ years of trying a new food every weekend and you’d expect my diet to be all normal and varied with only a few restrictions. Haha I wish. I’m pretty sure after all this time it has gotten worse. I guess the problem really is that my body thinks pretty much everything other humans call edible is unfit for consumption, and it lets me know that loud and clear.
That all is the much needed background to my current diet. I guess I should share what it looks like at some point as that is the main reason I wrote this article, so here goes:
Breakfast
3 cups of cooked rolled oats with ½ sliced banana and ½ cup blueberries.
1 Orgain Nutritional Shake
Snack
1 Orgain Nutritional Shake
Lunch
2 cups of cooked buckwheat, ½ sliced banana, and ½ cup blueberries
1 Orgain Nutritional Shake
Dinner
2 cups of cooked buckwheat, 1 ½ cups cooked broccoli, ½ a cooked chicken breast.
So…..yeah. I’ve pretty much been eating that or some slight variation (I used to eat a lot of plantains too) day in and day out for a few years now. Pretty messed up right? I am pretty sure from the outside this looks like at least disordered eating if not a full blown eating disorder. But, like, what am I supposed to do? It's not like I am not trying to expand my diet, I just can’t without Crohn's kicking my butt. Also I promise I’ve told every GI doc I’ve had about this and unfortunately there hasn’t been anything they have been able to do to help.
I decided to write this article because during the few years I’ve had these issues with all these trigger foods I’ve never really found anything online that mirrors what has happened to me. My hope is that if there are more people with IBD out there who struggle with these food issues as much as I do, that you at least feel validated that you aren’t the only one going through this. It sucks, and maybe one day we will have an answer as to why it happens.
Until then, if you are having issues with foods triggering your disease, bring it up to your doctor or dietitian. Spread the word. Even if, like in my case, the doctors or dietitian isn’t able to fix the problem, at least we are fostering awareness and discussions that will bring about solutions in the future.

Digestive Disease Week: Positive Gluten Sensitivity Seriologies and the Impact of Gluten Free Diet in Patients with IBD
There are a lot of strong opinions surrounding gluten free diets. Some view them as a fad diet, popularized by media and celebrities. Others report real improvements in their GI symptoms when going gluten free. And of course there are those with Celiac Disease, for whom a gluten free diet is a life changing therapy. Throughout my time as an undergrad studying dietetics, I have learned about the gluten free diet from all angles. I think a lot of the confusion surrounding the gluten free diet in IBD comes from two sources. First, there appears to be a difference between what patients report and what the limited research has shown. Second, this limited research and lack of conclusive evidence has created a difference of opinions among healthcare professionals themselves. It is a difficult situation where providers using their clinical judgement can recommend for or against IBD patients going on a gluten free diet, and both recommendations would be completely justifiable.
In this article, I plan to give some background on the gluten free diet, and the current evidence for and against its use for patients with IBD. Then, I will summarize the wonderful study I learned about during DDW 2021 presented by Dr. Maria Moomal Dahar titled: Positive Gluten Sensitivity Seriologies and the Impact of Gluten Free Diet in Patients with IBD.
What is a Gluten Free Diet?
Gluten free diets are designed to eliminate the protein gluten from one's diet. Gluten is a storage protein found in some grains, including wheat, barley, and rye. Gluten is an important protein for baked goods, as it forms a sticky network that gives dough its characteristic stretch and elasticity. I don’t want to go too much in depth, as there is already an amazing article on the CCYAN website written by Leah Clark that describes the gluten free diet. If you desire to learn more about the specifics, her article can be found here.
The Gluten Free Diet and IBD
The main reasons to follow a gluten free diet are Celiac Disease, non celiac gluten sensitivity, and wheat allergy.
Previously, there had been conflicting data regarding whether IBD patients are at a higher risk of developing Celiac Disease than healthy people. Some older, smaller studies have found increased risk, while others have found no increased risk or even decreased likelihood of having Celiac Disease.1 A recent, larger study has shown that IBD patients have an increased risk of having celiac disease.
Non celiac gluten sensitivity is characterized by abdominal pain, discomfort, bloating, changes in bowel habits, fatigue, or depression after consuming gluten. The prevalence of non-celiac gluten sensitivity in IBD patients surveyed is reported to be between 5-28%.1 Those IBD patients who reported non-celiac gluten sensitivity were more likely to be following a gluten free diet. One thing I found interesting was that IBD patients were more likely to report gluten sensitivity if they also had a flare in the past 60 days. This points to the possibility that gluten sensitivity might be worsened in patients who are currently flaring or who have recently had a flare up of their IBD.
Most research on the gluten free diet in IBD patients has been done through survey based studies. Unfortunately, these types of studies can only provide weak evidence at best. The surveys did find that of IBD patients who had tried a gluten free diet, about 2/3 reported an improvement in one of abdominal pain, bloating, diarrhea, nausea, or fatigue. About 40% of patients following a gluten free diet reported less severe or less frequent flares. Contrary to those positive results, a different survey study found that there were no significant differences in disease activity, hospitalization, or rate of surgery in IBD patients following a gluten free diet versus those who were not.
A few different organizations and guidelines have weighed in on the gluten free diet and IBD:
The International Organization for Inflammatory Bowel Diseases currently states that in IBD “there is insufficient evidence to recommend restriction of wheat and gluten.”
The Crohns and Colitis Foundation states that “some IBD patients have found that a gluten-free diet reduces their symptoms, but researchers have not proven that it reduces IBD inflammation.”
The Asain Working Group guidelines on diet and inflammatory bowel disease state that “a gluten-free diet is not of a proven value in patients with inflammatory bowel disease.”
There are also some confounding factors when discussing gluten free diets. Gluten is often paired with fructans in foods, which are a type of fermentable carbohydrate that is associated with gastrointestinal symptoms. One study showed that 80% of patients with suspected non-celiac gluten sensitivity couldn’t be diagnosed after a gluten challenge.2 This points to the possibility that something found alongside gluten might be the culprit. Fructans offer a convincing alternative cause for why some might experience GI symptoms while eating gluten containing foods. Indeed, research has shown that in patients with suspected non-celiac gluten sensitivity, eating fructans was associated with more gastrointestinal symptoms when compared to eating gluten.3
Positive Gluten Sensitivity Seriologies and the Impact of Gluten Free Diet in Patients with IBD
When I first noticed this study as a part of DDW I was excited. I think that the study design is well thought out. The term “Celiac serologies” means that antibodies to proteins associated with consuming gluten were found in patients’ blood. These patients have immune systems that have already falsely identified these specific proteins as foreign invaders. By studying patients with positive celiac serology, the researchers were able to look at the effect of a gluten free diet in the patients that were likely to experience the greatest benefit from going gluten free.
The goal of this study presented by Dr. Maria Moomal Dahar was to determine if there were any differences in clinical outcomes between IBD patients with positive celiac serologies following a gluten free diet compared to those who were not following a gluten free diet. Out of the 1537 patients IBD patients looked at, only 89 had positive celiac serologies. Of these 89 patients, 29 reported adhering to a gluten free diet.

One interesting finding was that of the 89 patients with positive celiac serologies, those who were not on a gluten free diet were more likely to have a high ESR (measure of inflammation) and eosinophilia (associated with inflammation and infection).
Based on this study, the authors recommend testing for celiac serologies in patients with IBD. They also suggest a trial of a gluten free diet in IBD patients with confirmed celiac serologies.
My Closing Thoughts
It is so important that research is being done to evaluate the gluten free diet in IBD. Any time where a large majority of patients report improvement following a dietary trend, that should at least warrant some investigation into whether or not those improvements can be replicated in a randomized controlled trial. I am thankful for researchers like Dr. Dahar and her colleagues who are making efforts to further our knowledge in regards to the gluten free diet and its use in IBD.
One thing I also want to note is that the majority of therapeutic diets studied in IBD (IBD-AID, CDED, EEN, and SCD) all exclude gluten containing grains. Some of these diets show real promise in treating inflammation or alleviating symptoms of patients with IBD, and it is a trend worth noting. On the contrary, the mediterranean diet has also shown similar promising results, and includes gluten containing grains.
In my opinion, current literature is frustratingly inconclusive. Like many nutrition topics, there isn’t enough evidence to be able to make any strong recommendations one way or another. In light of that, I think that the best approach is the same one I echo all the time: Find out what works for you individually. You know your own body better than any study, scientist, or doctor ever will. So if you notice feeling better on a gluten free diet, maybe that is something you decide you want to continue even if the evidence isn’t quite there yet to show benefit in IBD patients.

Meal Replacements and Oral Nutrition Supplements
Sometimes eating sucks. When my body hurts, I'm tired, and my gut is bloated, the last thing I usually want to do is add fuel to the fire by eating a meal. This is an unfortunate situation to be in because eating is one of those things we kind of have to do to survive. Luckily, there is a way to meet our needs without really eating. Enter the oral nutrition supplement. Calorie dense nutrition shakes designed to give you all the vitamins and minerals you need for livin’ in as little volume as possible. You can down one of these bad boys in under a minute and not have to worry about figuring out how you might fit an entire meal in your distended abdomen.
There are a lot of different nutrition supplements on the market, and it can be difficult to try to figure out which to buy. There are so many factors to consider, it can almost be overwhelming. In this article, I have tackled a few of the more common factors people consider when looking for supplements. Hopefully I have been able to provide some clarification on the differences between some of the common choices for meal replacement shakes.
Calories
The amount of calories I look for in one of these supplements depends on why I am using it in the first place. Am I trying to replace a meal? Then I would probably reach for something with a higher amount of calories. I usually try for at least 250 calories per shake, but closer to 500 calories is probably better. If I am using the shake to replace a snack, maybe 200-300 calories would be more desirable.
Some nutrition supplements come as a powder that you can mix with water or another liquid. The benefit of these supplements is that you can add as much powder as you want and customize the amount of calories to the situation. Products like Modulen IBD, Huel, Garden of Life Raw Organic Meal Shake, and Super Fuel all come as mixable powders. Garden of Life is one of the lowest calorie options I have seen, coming in at 120 calories per serving.
Most ready to drink supplements also have higher calorie options available. Ensure and Boost both make higher calorie versions of their regular nutrition shakes. You can usually tell a higher calorie shake because it will have the word “plus” in the name, i.e. Ensure Plus or Boost Plus. The big downside of these higher calorie versions is that a lot of the extra calories come in the form of sugar.
Fat
Fat is a tricky one. Often demonized, fat plays an important role as a source of energy, absorption of certain fat soluble vitamins, and managing inflammation. Certain fats are even essential, which means that we must get them from our diet. The type of fat in nutrition supplements matters. In most supplements, the fat content will be from vegetable oils. Animal fats are unusual or minimally used due to their tendency to be solid at room temperature.
Certain fats in vegetable oil, such as the Omega 6 fatty acids, are sometimes mis-labeled as pro-inflammatory. While these fats can be used by the body to create inflammatory molecules, research has shown that omega-6 fats are associated with lower or unchanged markers of inflammation. If you are somebody who is concerned about these fats, choose a supplement higher in monounsaturated fats such as Orgain or Huel. Looking for the words “high oleic” in the ingredients list is a good way to know that the oil used is high in monounsaturated fats. One supplement, Super Fuel, actually lets you add the fat to your shake yourself, so you can choose the exact type of fat you want!
Carbohydrates
There are a lot of considerations when looking at the carbohydrates in nutrition supplements. Some of the important things in my opinion are the sugar content, presence of artificial sweeteners, presence of maltodextrin, and fiber.
Sugar is an interesting one. The International Organization for the Study of Inflammatory Bowel Disease (IOIBD) says in their guidelines that there is insufficient evidence to recommend any specific change of intake of complex carbohydrates or refined carbohydrates or refined sugars and fructose. Therefore, any reason to limit sugar would have to be based on the known effects of high sugar consumption on heart health, gut health, weight gain, and other markers of health. Many of these supplements are high in added sugars, so it might be prudent to look for some of the lower sugar options such as Super Fuel, Huel, Orgain, or Garden of Life.
Some supplements contain ingredients that might be harmful in IBD patients. Specifically, maltodextrin and artificial sweeteners. Some of the low sugar supplements, such as Premier Protein, use artificial sweeteners like sucralose to replace sugar as a source of sweetness. Most supplements found in stores, including Ensure, Boost, and store brands such as Equate contain maltodextrin as a source of carbohydrates. In the IOIBD guidelines, the researchers note that it may be prudent to limit intake of both maltodextrin and artificial sweeteners. The authors also note, however, that the evidence for maltodextrin is theoretical and mostly based on animal models. Nutritional therapies that involve consuming nutrition supplements with maltodextrin have been found to be effective in IBD, so the jury is still out on maltodextrin.
Fiber is also a hot topic in IBD. Many foods considered healthy contain fiber, but many IBD patients who are flaring consider fiber to be something that aggravates their disease. Many of these supplements contain very small amounts of fiber, usually between 1-2 grams per serving. Some supplements, such as Huel, Kate Farms, and Super Fuel contain a higher amount of fiber. The general consensus from what I have researched appears to be that if you tolerate fiber, more is better. Like many other factors in IBD, fiber seems to be something to consider on an individual basis. Of note, Walmart’s brand Equate was the only supplement I looked at that had 0 grams of fiber per serving.
One thing to note is that some supplements include blends of fruits, vegetables, and other plant compounds. Orgain, Garden of Life, and Kate Farms all include these special blends, likely to try to mimic the benefits of eating whole foods. Other supplements, such as Huel and Super Fuel are made primarily from whole foods.
Protein
The protein needs of an IBD patient are increased during a flare. Protein is needed to help repair damaged tissue and maintain muscle mass, among many other functions. I think it is important to make sure that the nutrition supplement you choose has the protein your body needs to function optimally.
Most supplements have enough protein to meet your body's needs. A little trick I use is to try to shoot for 20% of calories from protein. You might need to whip up your phone calculator in the store, but the math isn’t too hard. First you would take the grams of protein and multiply it by 4, because there are 4 calories in every gram of protein. Then, all you need to do is divide the number of calories of protein by the total calories and multiply by 100 to get the percent!
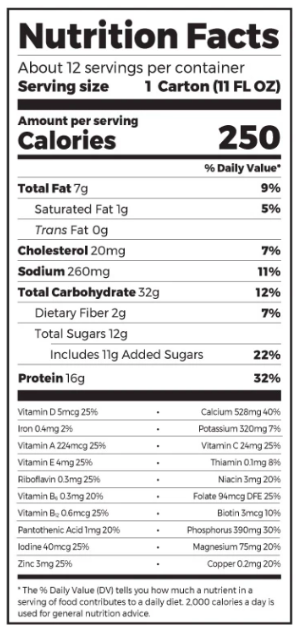
Let's do an example with Orgain’s Nutritional Shake:
Looking at the bottom, we see Orgain has 16 grams of protein per serving.
Step one would be to multiply 16g by 4 to get the number of calories, which would be 64 calories of protein.
Step two, would be to divide the number of protein calories by the number of calories in a serving, which can be seen at the top of the nutrition facts label.
We would do 64 calories divided by 250 calories and get 0.256.
The final step, to get a percentage, would be to multiply by 100 to make that number a percentage. So, .256 multiplied by 100 is 25.6%.
25.6% is more than 20%, so Orgain would pass my little test!
Some of the higher protein supplements out there are Huel, Ensure Enlive, and Premier Protein, and Garden of Life. It is important to note that if you aren’t in a flare, your protein needs are likely no higher than the rest of the population.
Carrageenan
Carrageenan is an emulsifier used to help the ingredients in shakes mix smoothly. It has also been shown to cause a variety of negative effects in animal models, such as increased blood in stool, increased inflammatory markers, and lesions in the bowel. For these reasons, and some small scale human research, IOIBD also states that it may be prudent to reduce intake of processed foods that contain carrageenan in both UC and Crohn’s Disease. Most of the supplements found in stores, such as Ensure, Boost, and store brands such as Equate use carrageenan in their nutrition supplements. If carrageenan is something you wish to avoid, you can usually locate it at the bottom of the ingredients list. You can see it is the last ingredient in Ensure Plus.

To Conclude
I wish I could add more detail, but I don’t want to break your scroll wheel. The most important thing to do when looking for an oral nutrition supplement is to take a look at the nutrition facts label and make sure you are comfortable with the nutrition content and ingredients in your shake. I usually try to look for higher protein and fiber, and lower added sugars while avoiding sucralose, maltodextrin, and carrageenan. Oh and the shake has to taste good too. Could you imagine not wanting to eat anything and reaching for a shake that didn’t even taste good? Neither could I. Considering all that, I usually go for Orgain nutritional shakes. They fit my goals as far as cost, taste, and nutritional content are concerned.
Another option is to try to make your own shake in a blender. It can be pretty easy to toss some oats, a banana, and a few scoops of peanut butter together and have a tasty, nutritionally dense smoothie to sip on. You even save some money that way too! At the end of the day, store bought shakes or homemade, oral nutrition supplements can be a great way to give your body the fuel it needs to function when you don’t feel like making or eating a meal.

What is a Healthy Diet?
Back when I was in college, I had a professor who hated the word “healthy”. She argued that the word had no real definition. At first, I am not sure if I agreed with her. Surely it was safe to say that something like spinach was a healthy food, right? It has fiber, loads of vitamins and minerals, and is low in calories - perfect health food! As time went on, and I thought about it more and more, I discovered she was right. There really is no one definition for the word healthy, because it applies differently to each of us.
Every person has their own goals as far as their health. For a bodybuilder, gaining muscle might be considered healthy. For a sprinter, something healthy might improve their times on the track. For others, healthy is eating in a way that will help extend their life. You can see that it isn’t as simple as slapping the label “healthy” on a food and calling it a day.
One of my favorite examples is birthdays. It doesn’t take a nutrition expert to know that birthday cake doesn’t improve physical health, but what about mental health? The goal on birthdays has never been to help you sculpt that hot summer body, but rather to celebrate with friends and family. It is a time to feel joy that we have made it another year on this Earth. If taking the birthday cake away harms that goal, well then the only conclusion I come to is that birthday cake is health food. Don’t tell anybody at the hospital I work at I just wrote that.
What about for people with IBD? What does a “healthy” diet look like for us? Having an interest in nutrition as well as IBD, I wrestle with this question a lot. I know that for the general population, foods like broccoli and brussel sprouts have been shown to reduce cancer risk, among other benefits. Therefore, they would generally be considered “health food”. But for somebody in an IBD flare, you might be better off roasting a package of nails at 350 in the oven for dinner. All that roughage is just going to result in pain and irritation as it passes through the inflamed intestine. For an individual with IBD who is in a flare, broccoli and brussel sprouts might be the furthest thing from healthy food they can eat.
That is why I think it is so important that we all understand the temporary and individual nature of the word healthy. It is not set in stone, what is healthy for you to eat today might not be healthy for you tomorrow. You should never be ashamed because you are not eating what the average person would call a “healthy” diet with this disease. That isn’t to say that you shouldn’t pay attention to diet at all. Your definition of a healthy diet will depend on your goals, which will most likely be very different from the friends, family, and coworkers you interact with on a day to day basis. Don’t compare apples to oranges. Take the time to define your health goals, and then determine what foods will help you reach those goals. Find your healthy diet.
IBD Diets: Gluten Free for Crohn's and Colitis
By Leah Clark
Because of the popularity of Hollywood fad diets, the term 'gluten-free' has become more and more popular over the past decade. While not necessarily intending to do so, this trend actually brought great change to individuals suffering from celiac disease, non-celiac gluten sensitivity, and inflammatory bowel diseases. With new food products coming to market and more menu items coming to restaurants, it has provided a new way for people that cannot eat gluten to experience food. As someone that was diagnosed with both celiac disease and #Crohn's disease ten years ago, I can confidently say I know my way around a nutrition label. That being said, not everyone that is on a gluten free diet, or that is planning on starting one, knows what to do. When discussing your treatment plans for your IBD with your doctor, discussing diet changes should not be forgotten. So, is going gluten free right for you?

Bacon, eggs, potatoes...who says living a gluten free lifestyle means giving up your favorite breakfast foods!
What is gluten?
With all these terms of gluten free, gluten sensitive, wheat-free, gluten-friendly, and more, it can be confusing to know what it all means! Isn't flour gluten, or is it any grain? To start with the basics of a gluten free diet, one has to know what to look for. Gluten is the proteins found in wheat, rye, and barley. So when on a gluten free diet, wheat, rye, and barely are the foods to avoid.
How to read labels
Okay, so know that I know what to avoid, what are the necessary steps to ensure that I don't eat the wrong foods? Check labels on everything. Even if you think something may be gluten free, it never hurts to read the nutrition labels. Certain foods don't have labels, such as fruits and vegetables; however, these foods do not consist of any other ingredients other than what they are called-apples, carrots, oranges, etc. Foods that are made with other ingredients, such as cereal, pasta, and crackers, are foods that need to be checked. Luckily, most companies are good about food labeling, so boxes will often say "Gluten Free" or "Contains: milk, soy, and wheat."
However, sometimes there are tricky labels that you need to look out for. For example, the cereal Rice Krispies is not #glutenfree. The ingredients include rice, sugar, salt, malt flavor, and vitamins and minerals. The key word here is malt. Although the other ingredients are okay, the malt flavor is not. Malt is a tricky word because it is not wheat, rye, or barely; however, malt is a derivative from barley. Therefore, Rice Krispies are not gluten free. Words like malt extract, malt flavoring, barley malt, wheat-germ, and non-gluten free oats, are words to look out for.
What foods can I eat?
A good rule of thumb is to stick to foods that are labeled gluten free, or are"natural" foods. By natural, I mean foods that are not made with large amounts of ingredients. A good starting gluten free grocery
list could include:
Fruit-apples, bananas, kiwi, oranges, grapes, strawberries, raspberries, blueberries, plums
Vegetables-carrots, corn, green beans, lettuce, spinach, broccoli, radishes, celery, zucchini
Milk-can be almond, dairy, soy, cashew
Protein-lean meats, chicken, eggs
Dairy products-cheese, gluten free yogurt, butter, cottage cheese
Grains-white or brown rice, gluten free oatmeal, gluten free breads and pastas

Gluten free pizza? Yes please! Restaurants have gotten better at properly preparing gluten free dishes, including delicious pizza, to make it easier for people to enjoying going out to eat.
Gluten free diet can not only be good for your gut, but also for other parts of your body because of how healthy a gluten free diet can be. Many of the foods listed are healthy in their nature, like lean meats, fruits, and vegetables. However, just because something says "gluten free," does not mean it is part of a healthy diet. Sure, chocolate is gluten free, but if all you ate was chocolate, would that be the best way to go on a gluten free diet? Probably not.
But I thought gluten free foods always tasted bad?
A common misconception about gluten free food is that it tastes gross. While yes, there are some bad gluten free food products out there, this is no different than there being bad gluten food. It all depends on your preferences and experimenting with different brands. Making home-made gluten free brownies is not as simple as using a Pillsbury box recipe of 'normal' brownies (although, there are some Pillsbury gluten free baking products that taste great). The point is to try new brands and baking techniques that work for you. I've spent the last ten years of my life finding my favorite brands of pastas, crackers, and bread, and I can honestly tell you, it wasn't I traveled to an entirely different country and tried their gluten free bread that I found my favorite. Gluten free food can taste just as good, if not better, than the food you're used to! It just takes some time and preparation.
How do I know if gluten free is right for me?
Honestly, it all depends on what you and your doctor think is best for you. I had to go gluten free because I was diagnosed with a disease that literally required me to. Yet, I know several people with Crohn's or colitis that have gluten free diets that do not also have celiac disease. In short, if eating certain foods make you feel bad, do not eat those foods! There are other foods I avoid even though they are gluten free, such as popcorn and caffeinated sodas, because I know they upset me. It truly depends on each person and if it is going to help with your treatment for IBD.