

NEWS

Digestive Disease Week: Role of Diet, Lifestyle, and Environment in IBD
I thoroughly enjoyed attending Digestive Disease Week’s session on Role of Diet, Lifestyle, and Environment in Inflammatory Bowel Disease. Let's start from the beginning and understand why studies surrounding diet, lifestyle, and environment are so important in understanding IBD.
IBD affects nearly 3 million Americans and over 200,000 Canadians. IBD is an immune-mediated disease that occurs due to certain, unknown environmental exposures in those with underlying genetic predispositions. Research on environmental exposures is needed to discover what environmental factors may contribute to an individual receiving an IBD diagnosis. This research will not only create an overall improved understanding of IBD, but also contribute to reducing the onset of IBD as well as cures for IBD.
Ultra-Processed Foods and Risk of Crohn’s Disease and Ulcerative Colitis
Two speakers in this session I found extremely interesting, the first being Dr. Chun-Han Lo. Dr. Lo reviewed his study on ultra-processed foods and risk of Crohn’s Disease and ulcerative colitis. The Western diet is thought to increase the risk of IBD through changes in the gut microbiome which can trigger immune function when compared to the Mediterranean diet.
Foods were separated into four categories from least to most processed:
Unprocessed
Processed culinary ingredients
Processed foods
Ultra-processed food products
Dr Lo explains that right now, it is widely known that higher consumption of ultra processed food products is associated with all-cause mortality, cardiovascular disease, metabolic syndrome, obesity, and cancer. Agents and thickeners, that are often added to ultra-processed food products, were also examined. The study aimed to examine the associations between ultra-processed food products and the risk of incident of Crohn’s Disease and ulcerative colitis.
The results indicated that higher consumption of ultra processed food products, specifically ultra processed grain foods and fat and sauces, was associated with an increased risk of Crohn’s Disease. Additionally, emulsifiers and thickener containing foods increased the risk of Crohn’s Disease. No subgroups had an association with risk of ulcerative colitis. This differentiates the impact food may have on Crohn’s Disease versus ulcerative colitis, furthering complexifying IBD. Further studies are needed on the effect of ultra processed food products in patients with established IBD may be warranted.
Although you may not be surprised by the results, studies like these are so important to allow room for more niche research and continue to allow researchers and doctors to understand the WHY behind IBD. As a Crohn’s Disease patient with many food intolerances, I am excited to see research surrounding diet and quality of food. There is little research backing the quality of food, and many suggest following a specific diet such as low FOD-map, gluten free, dairy free, among many others. It’s extremely exciting to see additional research surrounding foods, specifically processed versus unprocessed foods. My hopes are that this study can contribute to encouraging people to eat better quality foods and, in turn, reduce Crohn’s Disease diagnoses. Further, my mind jumps to future research covering whether reducing ultra processed food products after an IBD diagnosis could help treatment and management of disease.
Development of a Composite Environmental Score to Predict Age of Onset and Outcomes in IBD
Dr. Nidah Shabbir Khakoo spoke on the development of a composite environmental score to predict age of onset and outcomes in IBD. Specifically, Dr. Khakoo focuses on the fact that many environmental exposures associated with IBD are increasingly seen with Westernization. The study aimed to explore the relationship between individual environmental exposures and the age of onset of IBD. This study is extremely important in order to come to the understanding of what can cause a person to be diagnosed with IBD earlier in life, rather than later.
As someone with IBD, I have frequently wondered what environmental exposures in my life have caused my IBD to have an earlier onset? Why did I receive my IBD diagnosis in my early twenties compared to others that are diagnosed in their fifties? These studies are crucial to understand potential causes for earlier disease onset and overall understanding of IBD.
This study was administered on adult patients previously diagnosed with IBD. An environmental survey that queried age-dependent and lifetime exposures to various environmental factors were given among the participants to identify the environmental exposures each subject has had throughout their lifetime while looking at the age of their diagnosis. It is important to note that this study had a large number of hispanics, an underrepresented group in IBD research. The study looked at the age of disease onset, specifically comparing hispanics vs non-hispanics and Crohn’s disease vs ulcerative colitis patients.
Earlier Ulcerative Colitis Onset:
US Born
C-section Delivery
Fewer bathrooms
Decreased housing density
Ex-smokers
No farm contact
Earlier Crohn’s Disease Onset:
US Born
Water source - plastics
Fewer bathrooms
Decreased housing density
Smokers
Dr. Khakoo shares that the environmental score presented explains a greater amount of the variation in the age of UC onset than Crohn’s Disease onset. Additionally, weighted and not-weighted scores did not predict disease location, presence of extraintestinal manifestations, likelihood of surgery or hospitalization, or number of biologics needed. Certain environmental exposures, such as bottle feeding, showed opposing effects in ethnic groups with IBD, leading to assume that cultural and socioeconomic factors may influence disease onset.
These results give a baseline that other research needs to build off of. It is becoming increasingly evident that ethnicity differentiates environmental factors contributing to IBD and more research is needed to understand these differences. I’m looking forward to hearing of future studies regarding this subject and am hopeful more nuances regarding environmental exposures and the timing of IBD onset will be discovered.
It was great to hear from multiple experts about diet and environmental factors relating to IBD. I think that the data so far shows that there is a lot of work to do to understand what environmental factors contribute to IBD. I am looking forward to seeing future studies dive more in-depth to discover the causes of IBD. I am incredibly grateful to have heard from Dr. Chun-Han Lo and Dr. Nidah Shabbir Khakoo, and am confident these studies will have a large influence on future research on Inflammatory Bowel Disease.

What is a Healthy Diet?
Back when I was in college, I had a professor who hated the word “healthy”. She argued that the word had no real definition. At first, I am not sure if I agreed with her. Surely it was safe to say that something like spinach was a healthy food, right? It has fiber, loads of vitamins and minerals, and is low in calories - perfect health food! As time went on, and I thought about it more and more, I discovered she was right. There really is no one definition for the word healthy, because it applies differently to each of us.
Every person has their own goals as far as their health. For a bodybuilder, gaining muscle might be considered healthy. For a sprinter, something healthy might improve their times on the track. For others, healthy is eating in a way that will help extend their life. You can see that it isn’t as simple as slapping the label “healthy” on a food and calling it a day.
One of my favorite examples is birthdays. It doesn’t take a nutrition expert to know that birthday cake doesn’t improve physical health, but what about mental health? The goal on birthdays has never been to help you sculpt that hot summer body, but rather to celebrate with friends and family. It is a time to feel joy that we have made it another year on this Earth. If taking the birthday cake away harms that goal, well then the only conclusion I come to is that birthday cake is health food. Don’t tell anybody at the hospital I work at I just wrote that.
What about for people with IBD? What does a “healthy” diet look like for us? Having an interest in nutrition as well as IBD, I wrestle with this question a lot. I know that for the general population, foods like broccoli and brussel sprouts have been shown to reduce cancer risk, among other benefits. Therefore, they would generally be considered “health food”. But for somebody in an IBD flare, you might be better off roasting a package of nails at 350 in the oven for dinner. All that roughage is just going to result in pain and irritation as it passes through the inflamed intestine. For an individual with IBD who is in a flare, broccoli and brussel sprouts might be the furthest thing from healthy food they can eat.
That is why I think it is so important that we all understand the temporary and individual nature of the word healthy. It is not set in stone, what is healthy for you to eat today might not be healthy for you tomorrow. You should never be ashamed because you are not eating what the average person would call a “healthy” diet with this disease. That isn’t to say that you shouldn’t pay attention to diet at all. Your definition of a healthy diet will depend on your goals, which will most likely be very different from the friends, family, and coworkers you interact with on a day to day basis. Don’t compare apples to oranges. Take the time to define your health goals, and then determine what foods will help you reach those goals. Find your healthy diet.

Calling in Sick and IBD
Hustle culture - committing your life to your job and career - has become normalized and even expected in young adults. After graduating university, many find their self worth linked to their career, earning promotions, competing with coworkers, and impressing your boss. As a twenty something year old with Inflammatory Bowel Disease, the struggle to balance work with your health is never ending.
Those with a chronic illness understand not to take life for granted and that each day can be as unpredictable as the next, but we often forget this and get caught up in prioritizing a career over our own health and wellbeing. Calling in sick to work is inevitable, everyone has to do it at some point in their lives, whether it’s for a mental health day, the flu, or a flare-up. Yet, there are so many negative stigmas around missing work and around prioritizing your body.
The feelings of guilt that come with calling in sick to nurture your body, whether you see your body deteriorating, know a flare is coming, or if a flare comes out of the blue, can be overwhelming. The stigma associated with hustle culture and calling in sick can feel disheartening. I have always had a hard time taking a sick day, and I always felt like I was letting my boss and coworkers down and that I wasn’t worthy of employment. Intense feelings of frustration and annoyance invaded my mind when debating whether to call in sick and these intrusive thoughts caused my body more stressors on top of being physically ill. I often remind myself that prioritizing my body is my number one job. Without my health, I wouldn’t have a job and I wouldn’t be able to participate in all the amazing experiences life has to offer.
A helpful comparison to calling in sick is the safety instructions reviewed when boarding a flight, right before take off. The flight attendant always reviews the emergency instructions, stating that if the plane were to lose oxygen, you are always to put on your own oxygen mask before helping someone else. Putting yourself first will enable you to not only succeed at your job, but also to succeed in other aspects of life. If you were to ignore your body’s signals that you need rest, you will become more sick and risk the most important thing, your health.
You are not weak, undeserving, or less important than your colleagues and friends because you need to call in sick more often than the average person. You are strong, resilient, and brave. We battle a viciously unpredictable disease that many do not understand. Do not let your worth be measured by whether you call in sick. I challenge you to listen to your body and honour what your body is saying, you never know how far you will fly until you respect and love yourself and with that includes respecting your body’s limits.
Recently, I took two sick days at work due to a small flare up and my boss and coworkers were overly supportive. Although feelings of guilt surfaced when I was making this decision, the second I returned to work, everyone showed how much they cared about my wellbeing.
If you are experiencing toxicity in the workplace, contact the Human Resources department. If your company does not have a HR department, set up a meeting with your boss or manager. If you continue to be pressured to not take sick days, to put your job before your health, this may be time to look for another job and boss that cares about you and allows you to put your health first.
On this note, being able to call in sick has undeniable privilege. Many people across the world are unable to call in sick without suffering financially or being penalized at work. Openly having these hard conversations during the hiring process or with your HR department will contribute to breaking the stigma and providing accommodations for those that are chronically ill. It’s important to speak with your boss or HR representatives regarding sick leave, paid sick days, and working from home options. Speak up to your government representatives and express the need for a handful of mandatory paid sick days across your province or state.

The Power of Music
I still remember the first time I listened to the song Where’d You Go by Fort Minor. It was June of 2016, and I had just recently been diagnosed with Crohn’s disease and finished my last semester of high school. It had been a semester of overcoming pain and fatigue to drag the shell of my body across the high school finish line. With those less than stellar circumstances, I was overcome with emotion hearing the lyrics describe in words exactly how I was feeling:
She said "Some days I feel like sh**,
Some days I wanna quit, and just be normal for a bit,"
I cried then, and I still tear up occasionally listening to the song and thinking back on that period of my life. That is the power of music, the ability of the songwriter to share their feelings in a way that connects with another human. It grants the comfort of knowing that others have experienced the same things you are experiencing now. That can be powerful for those of us with IBD, because it can be so easy to feel isolated and alone in our struggles.
Today, I want to take you through some songs I feel reflect the IBD experience for me. I encourage you to listen through the links as you read.
One song I keep going back to is Times Like These by Eden Project. The first verse starts out with what a lot of us feel sometimes:
It's been a long, long time
We've come a long, long way
No, I can't see the finish line, scared half to death, but that's okay
It's been a long, long night
After a long, long day
My body's aching, but I know somehow, my feet will find a way
I don’t know about y’all, but I can think of at least a dozen times I felt like this with my IBD. It can be so hard to try to imagine the finish line when the reality of your disease forces you to acknowledge the present instead of looking toward the future. And that is scary. When day and night you are exhausted just putting in the bare minimum effort, you can forget to look at the big picture. I don’t even have to tell you how much I relate to the body aching line. But the great part about this song is that it doesn’t end there. Near the end, the artist sings:
These are the times we will hold
In the silence, when I've given all of me
And it's alright that it's over
And I found fight, like a soldier coming home
In the silence, but I have never felt so free
The future's so bright, this is our time
And I'll live it how I dream
It is beautiful how the artist not only changes the lyrics to reflect the hope, but if you listen, the entire mood of the song changes as well. The tempo speeds up, the instruments are cheery, and there is a joy in the tone of the singer. I know when I had flares in the past, it didn’t feel like a time in my life worth remembering. But I do look back on those times in my life now and see how they shaped my future. I see how I was supported and loved by family and friends, and how it gave me a feeling of gratitude for every new day on Earth. Some days you won’t be able to see the finish line, but eventually you’ll look to the future and it will be so bright.
Another song I feel encapsulates the IBD experience is Mountain at My Gates by Foals. It starts out with this verse:
I see a mountain at my gates
I see it more and more each day
What I give, it takes away
Whether I go or when I stay
Doesn’t that just sound like the IBD experience? We have this mountain of IBD in front of us, and sometimes it feels like it takes away everything from our lives. The beautiful thing about this song is it is about overcoming that mountain. The second to last verse goes like this:
Oh, when I come to climb
Show me the mountain so far behind
Yeah, it's farther away
Its shadow gets smaller day after day
Sometimes our disease can just feel impossible to overcome. But one day we will come to climb, and we will have realized we have conquered that mountain. We will look back, and see all that we have accomplished. Whether it is overcoming a flare, graduating college, or just taking a shower this morning, we all have mountains ahead of us that are made more difficult to climb by our disease. That just makes the view that much better once we reach the top.
Please leave a comment with any song you felt has been an integral part of your IBD journey, I would love to give it a listen.

Overcoming Medical Trauma with IBD
I have anxiety.
I am afraid to speak up, almost all the time.
I press my nails hard into my palms when I think about why I said “How are you?” too quietly.
I bring this up because about one year ago, I had an allergic reaction to an infusion. I had been on this infusion for several months, almost a year at the time. At first, I stayed quiet about the symptoms I had been feeling for a couple of weeks leading up to it.
I think a part of me genuinely thought it was in my head. When people around you are constantly telling you your illness is your fault or that you look fine or that your symptoms are just your anxiety, you start to believe it.
It started with red, blotchy spots all over my skin. Some days were worse than others and eventually, I went to see a dermatologist who prescribed me a topical medication and I didn’t think anything of it except for the occasional feeling of shame when the spots became more visible.
At the infusion before my reaction, I remember just thirty minutes into it, I felt so sick. I could hear my heartbeat in my ears and everything felt slow. I remember trying to explain that I wasn’t feeling well and then downplayed it for just being tired because I’m used to doing that.
At my next appointment, the same thing happened. I started to cough and my lungs and throat felt itchy. I felt little ants all over me, starting at my feet all the way up to my chest. I stayed quiet still because I thought I was just making it up in my head until my nurse pointed out that I looked a little flushed.
When I got up to go to the bathroom to check it out, with the IV machine trailing behind me, I stared at the mirror in absolute shock when I saw welts the size of quarters flooding my skin and hives spreading quickly across my chest and neck. My mother who was with me became panicked and called the nurse who immediately notified the doctor.
I remember I started laughing hysterically because I was so afraid. The nurse quickly started Benadryl through my IV and I was just shaking because I felt so cold. The doctor was asking clarifying questions but they just sounded like echoes in my head. Eventually, the reaction subsided and I just layed there, stiff, with anxiety.
What I didn’t know was that ever since that day, anytime I go to an infusion or take one of my medications I am so afraid of it happening again. I got lucky that my nurse noticed something was wrong before it was too late, but I can’t help but wonder if I had just spoken up earlier I could have avoided all of this in the first place.
But I want to stress that it is not your fault for not speaking up. Sometimes it can feel like anxiety is taking control over your life but every day you struggle with anxiety and still choose life, you are the one taking control of your life.
I don’t feel guilty anymore for not speaking up then but now I understand that I deserve to speak up for myself now. I deserve to be heard. When it comes to your health, it is never just in your head. What I mean by that is whatever symptom you are feeling-- whether it be a physical manifestation of anxiety, racing thoughts, pain, discomfort-- those are all valid and not imaginative.
The next time you feel too anxious to speak up, just remember that you deserve to be heard.

This article is sponsored by Lyfebulb.
Lyfebulb is a patient empowerment platform, which centers around improving the lives of those impacted by chronic disease.

IBD, Mental Health, and Diet
Have you ever had a gut feeling before? Maybe you’ve had butterflies in your stomach when taking a risk, or felt something in the pit of your stomach when receiving bad news. Are these just idioms, or is there something else there? On my journey to become a registered dietitian, the connection between food and physical health is a common theme. Something we talk about much less is the connection between food and mental health. While Inflammatory Bowel Disease (IBD) is often thought of as a physical disease, the mental impact cannot be ignored. In my opinion, we don’t talk enough about the IBD and mental health connection, and we certainly don’t talk enough about how food can play a role in this aspect of our disease.
Mental Health and Gut Health
What does gut health have to do with mental health? Strap on your helmet, it's time for a crash course in the connection between gut health and the brain. The gut has over 500 million nerves, which serve as a two way communication system with the brain. If your gut isn’t happy, you better believe it is going to let its good friend the brain know about it. Our guts are also responsible for producing neurotransmitters, which help to regulate physical and mental functions of the body. One important neurotransmitter that regulates mood, serotonin, is produced 95% in the intestines! Another one, GABA, can be produced by the friendly bacteria in the gut, and can help reduce feelings of anxiety, depression, and fear.
Mental Health and IBD
As you can see, the gut and the brain are basically best buds. But what does that mean for people whose guts are broken more frequently than the McDonalds ice cream machine? Unfortunately, IBD patients are at an increased risk for developing anxiety and depression, and frankly, can you blame us? We are forced to bear the burden of a lifelong chronic disease, often being diagnosed during some of the most mentally vulnerable stages of our lives. High school is hard enough without explaining why you spend half of every class in the bathroom. It might seem like the connection between intestinal health and brain health is bad news, but there is a silver lining. If we can change the health of our gut, we can change the health of our brain.
Diet and Mental Health in Healthy Individuals
In healthy individuals, certain diets have been shown to increase feelings of wellbeing, reduce feelings of depression, and improve psychological health. Both individual foods such as fruits and vegetables, as well as dietary patterns such as the mediterranean diet, have been linked to these benefits. Some foods are also associated with worse mental health. Sugar has been linked with mood disorders and depression. Excess sugar consumption is also associated with dysbiosis, a shift in the composition of the gut bacteria from helpful to harmful species.
Diet and Mental Health in IBD
In a study presented at Digestive Disease Week 2020, researchers categorized IBD patients into two groups, a high sugar group (>100 grams per day) and a low sugar group (<100 grams per day). They found that those in the high sugar group had increased feelings of fatigue, trouble with social engagement, feelings of depression, and trouble relaxing compared to IBD patients in the low sugar group.
It is important to note that sugar containing whole foods such as fruit have been strongly linked to positive health outcomes, and should be considered differently than sugars from processed foods. Added sugars from processed foods such as soda or candy are associated with an unhealthy gut, and worse overall health.
I think this is such an important study, not only because it has practical implications for IBD patients, but also because it opens doors for patients to take control of their own mental health. I don’t think I've ever had a conversation with any GI doctor about mental health, despite the increased risk we carry with IBD. Until that changes, it is reassuring to know that we have the option to eat in a way that is associated with good gut health, and therefore good mental health.
References
Choi K, Chun J, Han K, et al. Risk of Anxiety and Depression in Patients with Inflammatory Bowel Disease: A Nationwide, Population-Based Study. J Clin Med. 2019;8(5):654. Published 2019 May 10. doi:10.3390/jcm8050654
Knüppel, A., Shipley, M.J., Llewellyn, C.H. et al. Sugar intake from sweet food and beverages, common mental disorder and depression: prospective findings from the Whitehall II study. Sci Rep 7, 6287 (2017). https://doi.org/10.1038/s41598-017-05649-7
Stranges S, Samaraweera PC, Taggart F, Kandala NB, Stewart-Brown S. Major health-related behaviours and mental well-being in the general population: the Health Survey for England. BMJ Open. 2014;4(9):e005878. Published 2014 Sep 19. doi:10.1136/bmjopen-2014-005878
Parletta N, Zarnowiecki D, Cho J, et al. A Mediterranean-style dietary intervention supplemented with fish oil improves diet quality and mental health in people with depression: A randomized controlled trial (HELFIMED). Nutr Neurosci. 2019;22(7):474-487. doi:10.1080/1028415X.2017.1411320
Brown K, DeCoffe D, Molcan E, Gibson DL. Diet-induced dysbiosis of the intestinal microbiota and the effects on immunity and disease [published correction appears in Nutrients. 2012 Oct;4(11)1552-3]. Nutrients. 2012;4(8):1095-1119. doi:10.3390/nu4081095

Celebrating Black History Month in the IBD Community
“Representation creates trust, so why aren’t there more people who look like me included in research and education?” This quote by Melodie Narain-Blackwell brilliantly describes the feelings that so many Black and brown IBD patients have. In recognition of Black History Month, what can we as a chronic illness community do to support our fellow Black IBD patients this month? Standing in solidarity with this marginalized community, helping amplify their voices, and acknowledging their experiences are ways to starting bridging those gaps.
It is important to support BIPOC patients by recognizing the additional barriers that minorities, especially those in the Black community, face when navigating medical care and public health. Historically, Black people have been marginalized, abused, experimented on, and underrepresented in medical trials and research. Being seen as easily disposable, Black people have had to endure the systemic injustices of medical discrimination and medical racism. Crohn’s and ulcerative colitis are chronic diseases that statistically occur less frequently in African-Amercian populations. Statistics also show that Black people are more likely to not have their symptoms believed or validated, which has ushered a crisis of misdiagnoses. It is clear that implicit bias and antiquated medical beliefs are factors in the hesitation that Black people experience in the medical field. This phenomenon has led to an inherent distrust of medical institutions and treatment in the black community. As IBD patients we understand that having the right diagnosis and starting treatment is vital for healing and longevity. This concern is magnified in the Black community due to the systemic injustices previously mentioned.
When I first started to become ill in 2019, I did have some internal generational trauma that made me hesitant when seeking medical care. After months and months of pain I finally decided to go to the hospital to get some answers. When speaking to the doctor about symptoms, I vividly remember feeling an overwhelming sense of unease rattle through my bones. What happens if my experiences and symptoms aren't taken seriously? How can I truly convey the severity of how I feel? Although I did not receive a proper diagnosis from the hospital, I was lucky enough to have the staff members at the hospital believe and validate me. I was privileged that this was not an overtly terrible experience, but it does not take away from any reservations I had, as well as the reservations that countless other Black people have.
We must acknowledge and hold space for Black people within the IBD community through advocacy. Having a diverse range of anecdotes and stories will only propel this community to further embrace the lived experiences of so many Black and brown people who are voiceless. Education and conscious activism will only lead to more positive intersectional change.
In recognition and celebration of Black History Month, here are a few black pioneers in the IBD community as well as Gastroenterology:
Sadye Beatryce Curry was the first female African-American gastroenterologist in the United States. On top of her endless list of accomplishments, she was a founding member of the Leonidas Berry Society for Digestive Disease as well as the first woman to be elected chair for the Internal Medicine Section of the National Medical Association.
Leonidas Berry was the first African-American gastroenterologist in the United States as well as a pioneer for the advancement of endoscopy procedures. Dr. Berry also invented the gastroscopy scope. Leonidas Berry has a passion for bridging the gap of racial problems in public health.
Gary Richter is a gastroenterologist and currently runs Consultative Gastroenterology in Atlanta, and has become the first African-American president of the Medical Association of Atlanta.
Melodie Narain-Blackwell is the founder of Color of Crohn’s and Chronic Illness (COCCI) which is a nonprofit focused on increasing quality of life for minorities who battle IBD and related chronic illnesses.

How to Start a Food Diary
Dear Diary,
Sometimes when I eat it feels like a herd of angry buffalo have taken up residence in my gut. The rumbling, the pain, and the regret are all too familiar at this point. Maybe I just shouldn’t eat at all. Maybe that would be best. I wish it could just stop…
Okay, I might not be talking about that type of diary, but I’ve had many days in my Crohn’s journey where that could have described me. Like many people with Inflammatory Bowel Disease (IBD), I have a frustrating mix of good days and bad days. It always baffled me how I could feel good one day, but terrible the next. I wanted to know why. This started my journey of paying closer attention to what I eat, and in turn, keeping a food diary.
Why a food diary?
Our environment is everything we come in contact with on a daily basis that isn’t us. The air we breath, the things we touch, and the food we eat all make up our outside environment. If nothing in our environment impacts a disease, it should feel the same every single day. For me, and many others with IBD, this just isn’t true. In this case, we must start looking at our environment as a source of triggers for our disease.
One of the largest parts about how we interact with our outside environment is what we eat. Every day we eat a variety of different foods, from a variety of different places, that have a variety of different health effects. For me, food was an easy place to start to try to figure out some of my disease triggers. I know what I am eating every day, so why not try to see if there is any connection between what I eat, and how I feel. This led me to food journaling, and it has been an invaluable resource in helping me navigate and manage my own disease. It has given me power.
Research also backs up this idea. In one study done in 2016, one group of Crohn's patients was told to exclude either the four food types they had the highest antibodies to, while the other excluded the four food types they had the lowest antibody to. The group that excluded the foods types to which they had the highest antibodies had significantly lower disease activity and significantly higher quality of life.1 We might not have access to antibody testing, but we can certainly try to figure out what foods are worsening our disease and quality of life.
How to write a food journal
There are three main things to consider when writing a food journal: what you eat, the time you eat, and how much you eat. With these three written down, you will be able to better make connections between foods and symptoms. Let's do an example: For breakfast this morning, you ate a bowl of oatmeal with blueberries, some bacon, and a cup of coffee (I know, I know, coffee isn’t exactly known for its stellar track record in collaborating well with IBD, but it's a made up example!) How would that look?
Tracking Symptoms
Symptoms are a little trickier. Say you have some pain in your lower right abdomen, how do you know what meal might have triggered you? Was it the meal you ate 5 minutes ago? 4 hours ago? The day before? For this we need to know a little bit about how long food takes to get to each different part of the intestines, also called the intestinal transit time. In a normal, healthy adult the following is accurate:
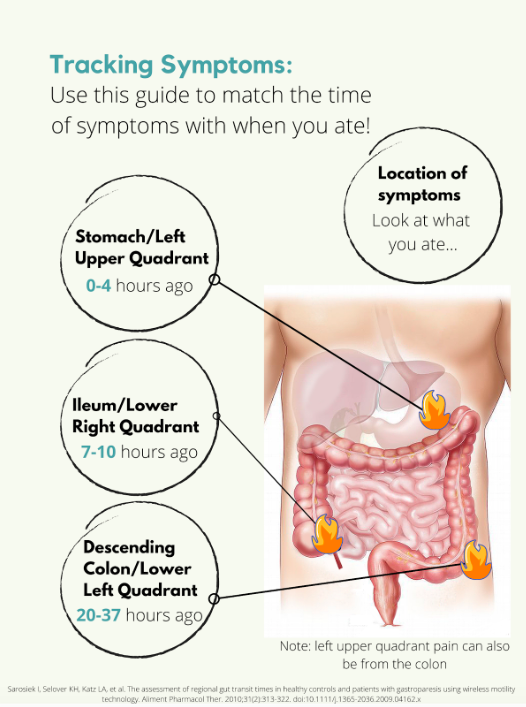
But what if you’re flaring? Diarrhea, inflammation, stricturing, and other aspects of a flare can all impact the amount of time it takes for food to get to the finish line. Some studies have been done on intestinal transit time in IBD patients, with most finding that the intestinal transit time is longer in IBD than in normal healthy subjects.2,3,4 In one patient with Crohn's disease, it took 156.2 hours for one meal to pass through. Talk about taking the scenic route! Like many other things with IBD, you are going to have to take an individual approach and problem solve to figure out how to best match symptoms and meals.
Resources
Tracking food can be done in something as simple as a spiral notebook, but there are also other options available. Here is a list of some apps you could use instead of a physical journal:
mySymptoms Food Diary & Symptom Tracker (Lite) by SkyGazer Labs LTD
Food Diary by WeCode Team
Cara Care by HiDoc Technologies
References
Gunasekeera V, Mendall MA, Chan D, Kumar D. Treatment of Crohn’s Disease with an IgG4-Guided Exclusion Diet: A Randomized Controlled Trial. Digestive Diseases and Sciences. 2016/04/01 2016;61(4):1148-1157.
Andersen K, Haase A, Agnholt J, et al. P-113 Gastrointestinal Transit Times and Abdominal Pain in Crohn's Disease. Inflammatory Bowel Diseases. 2017;23(suppl_1):S40-S41.
Fischer M, Siva S, Wo JM, Fadda HM. Assessment of Small Intestinal Transit Times in Ulcerative Colitis and Crohn's Disease Patients with Different Disease Activity Using Video Capsule Endoscopy. AAPS PharmSciTech. 2017;18(2):404-409. doi:10.1208/s12249-016-0521-3
Haase AM, Gregersen T, Christensen LA, et al. Regional gastrointestinal transit times in severe ulcerative colitis. Neurogastroenterology & Motility. 2016;28(2):217-224.

Advocating for the Specialized Care You Need: Reflections on Mount Sinai’s IBD Clinic
Recently, I’ve started receiving care from the Susan and Leonard Feinstein Inflammatory Bowel Disease Clinical Center at Mount Sinai. This was my first time visiting an IBD-specific clinic, ever. Prior to visiting Mount Sinai, I was lucky if there was a gastroenterologist or a colorectal specialist on call at my local hospital.
On my most recent visit to the IBD Clinic for a post-operation appointment, I thought I’d reflect on what made this center so special, especially during the COVID-19 era.

Post-surgery for an internal fistula -- feeling better already!
In light of the pandemic, the process for being admitted and seen (at any hospital!) has been streamlined into a tighter and safer protocol. With hand sanitizer stops at nearly every corner, I noticed that Mount Sinai took a heightened level of precaution than any other facility I had been in. Every doctor, nurse, and staff member had a face shield in addition to their masks, with some going as far as to don Bouffant caps.
Beyond the COVID-19 precautions, however, I would like to speak to the deeper and more important differences at this clinic -- the unspoken sense of solidarity between both patients and doctors alike. To have an entire facility devoted to this condition, a chronic illness shared by millions of Americans nationwide, means that there is a lack of cause to explain yourself. Everyone in the room is deeply familiar with the forms of IBD, along with all the embarrassing and critical details that few others are willing to talk about in their entirety.

The waiting room at the Mount Sinai IBD Center is all socially distanced!
This plaque, hung on the entryway of the floorwide clinic, is perhaps one of my favorite parts of the IBD Center. It’s a reminder of how fortunate we are, as young adults with IBD, to be treated in a time where our condition has been identified and researched, nevertheless with a name and prognosis. It is a strange feeling, indeed, to know that the work and medical achievements of this doctor (and his name!) has forever changed my life.

A plaque memorializing Dr. Burrill Crohn at the Mount Sinai IBD Center.
Of course, I would be remiss not to acknowledge how incredibly fortunate I am to live in the vicinity of this clinic. To have access to such a clinic with a focus on IBD in and of itself is a privilege, one that many Americans and patients are not so lucky to receive. I’m duly compelled, however, to point out how lacking our healthcare system is, especially for those suffering with chronic illnesses. As someone who was diagnosed with Crohn’s disease in the summer of 2020, a time when the SARS-CoV-2 virus revealed the greatest inequities and vast underpreparedness of American healthcare, I’ve come to meet, learn about, and further appreciate the frontline and essential workers, who are simply making the most of what they’ve got.
Although it took me months to find the right team of doctors and healthcare professionals, I learned that it was alright, and at times, even necessary, for me to ask for more specialized degrees of care. An important lesson in my brief yet transformative journey with IBD: don’t be afraid to advocate for the specialized care that you need.

Reflections: The Importance of Advocacy for IBD
It’s a little strange to title this article ‘Reflections,’ because IBD is unique in that it’s always ongoing, with nothing to really jump over and look back on to reflect; with the journey still very much running, our reflections are inbuilt into it.

As I write this, I’ve been in remission from ulcerative colitis for more than a year. From the time I was accepted to be a CCYAN fellow to now, I have already been through a rollercoaster of new emotions: from immense gratitude and relief that I am finally a fellow of a network that I closely followed for several months to staggering self-doubt about whether I can truly do this opportunity justice. While poles apart, my feelings of gratitude and self-doubt and the largeness of the two do stem from the same root. After I was diagnosed with UC at the age of 19, I desperately needed to know more people who faced the same struggles. With little else to focus on in those starting years, hope would glimmer every time I found out about a famous personality or someone I knew who opened up about their chronic illnesses.
The way an invisible chronic illness creeps up on young adults is very much like a thief breaking in your house when you’re asleep and stealing things that don’t seem so valuable at first sight but without which you can’t really survive (like all your dishes). As young adults, we are so entitled toward our bodies and organs functioning properly that there’s no way to prepare or even know you will be impacted and when you do, people have very strong opinions on what you could have done to avoid it. And if, like some organs, dishes weren’t replaceable and the upkeep of the damages was constant, the last thing anyone would want is to deal with the struggle alone and keep it private. At least that’s how I felt. As soon as I was diagnosed, I let everyone around me know mostly everything except for the “impolite” specifics. Sometimes if the gravity of my situation wasn’t acknowledged, I would push to reveal the impolite specifics too. Concurrent to my health challenges, I was still also learning aspects of a broad society I had entered just two years before I got UC. As I rushed to speak and be heard, I realized, through the fear of my family and the discomfort of peers and friends, just how closed this society is towards these things.
When there are no voices for something that drastically alters every aspect of your life, it feels as though you’ve been dropped off to a completely new city with no maps for guidance. Maps are important for not only getting you from point A to point B, but also giving you a sense of orientation to gauge where you are with respect to everything around you. No voices = no maps. By far, in India today, invisible illnesses not only lack visibility in patients' external bodies, but also in national and private datasets, policies, and advocacy. This leaves patients disorientated and vulnerable to quackery (health fraud), which results in the loss of crucial time, finances, and deterioration of mental health (with the ups and downs of new hope and disappointment).
If the silence around personal disturbances was anything to go by, then I did not do a very good job of fitting in to my society as I always took the opportunity to talk about what I was going through even when I realized with passing time that it wasn’t always welcome or understood completely. I thought I should speak up all the more, because if no one does, who will vouch for me? This casual monologue took greater form in my first experience of being at a public hospital in my city. By that time, I had scoured the internet for people like me, experiences like mine, unique symptoms like mine, etc. I had come to recognize some feelings that came as a by-product of my illness through Hank Green’s videos on YouTube, and that the illness was bigger than me and my doctors (who only focused on the strict textbook aspects of IBD). My mom and brother very supportively drove and accompanied me for my sigmoidoscopy and I even got to sit as I waited for my turn. Waiting for countless hours after the scheduled time of my appointment, I was busy drowning in my pond of self-pity. When I heard a young lady slightly older than me was invited to go before me, I was very irritated and urged my mom to leave and reschedule. My experienced mother knew better. As I waited, I could hear the conversation between the young patient and the doctors in the room next door. She was a daily wage worker and her grumbles about missing work, her stomach pain (due to which she tilted sideways when she walked) and the tedious hours she spent waiting for her turn followed her into the room. The doctors didn’t indulge her in any sympathy, but rather curtly started the process. I wondered out loud why they hadn’t offered her a sedative – whenever I was asked, I always thought what a preposterous thing to ask when the process was so intrusive and uncomfortable. It was because she was alone and needed to hear the doctor’s findings and, of course, had to head back home alone. Even in my miserable state, that struck something in me. Her yells and shouts during the process, and the surrounding patients’ aloofness painted a picture so bleak, I was forced to look beyond my situation and recognize that despair like mine was still placed high on privilege. Granted that sigmoidoscopies are not the most pleasant of processes to go through or even prepare for, her shouts seemed out of place. I gathered it was more of a release from the anxiety of being alone and in such a vulnerable position with no emotional support. It took me back to a brief, mostly one-sided exchange she and I had before she was called in. From the little I understood as she spoke rapidly in her dialect, she had absolutely no understanding of the formalities of the prep that had to be taken and, more worryingly, the seriousness of her illness. She had two kids she had to care for, and she came alone because her husband was a daily wage worker who could not miss work especially since she was missing work that day too. She complained to me about the high prices of prep, all the days she had missed getting tests done and scheduling and rescheduling appointments in a government hospital, her appetite loss due to nausea and how she couldn’t perform her labor-intensive work as efficiently. After she limped out of her session, I thought of the sheer population of people like her in India.
Ever since that episode, I started thinking beyond my illness and what I could do to help the numberless amount of people in the same boat as the young woman. To start helping, the first step is to get a clear picture of how many people are impacted by IBD, which is frustratingly not available nor acknowledged anywhere in India. I am grateful, therefore, that I found CCYAN as an international platform for advocacy. Advocacy would hopefully enable data collection somewhere down the line. However, sometimes the mountain looks too big to climb; at this moment, we are right at the bottom and there are many things to do. Sometimes I think of all the people suffering from IBD in India, and how many struggles go undiscovered due to health illiteracy, digital gaps, doctor unavailability, and expensive medication, etc. Now more than ever, as cases of autoimmune disease rise across the world, there needs to be a prominent force of advocacy for IBD in India, so that datasets can be recorded and informed policies can be formed. The innumerable people who struggle already for a living should not be further hindered in their struggle for support, information or resources in this regard.